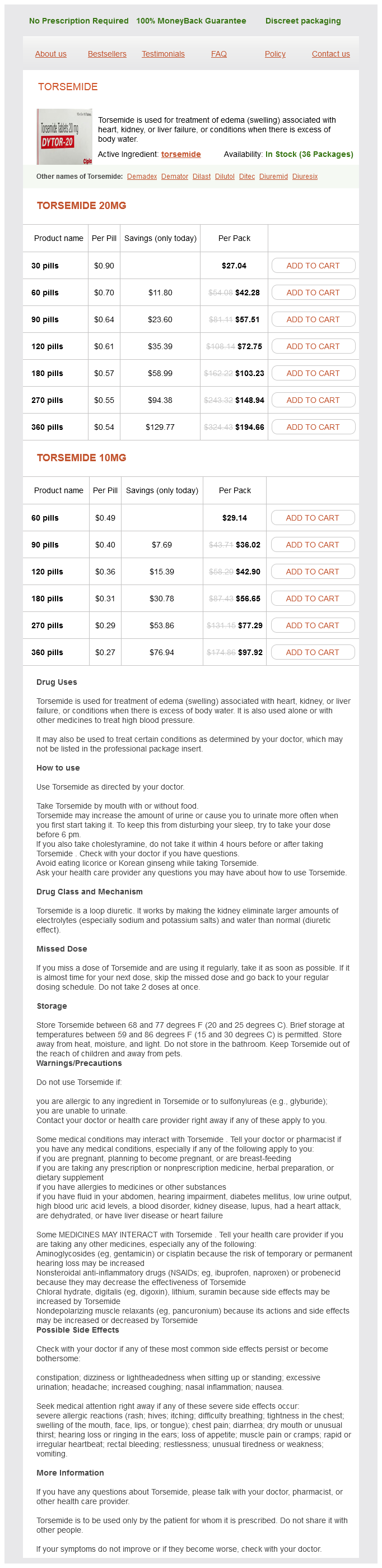
Torsemide 20mg
- 30 pills - $27.04
- 60 pills - $42.28
- 90 pills - $57.51
- 120 pills - $72.75
- 180 pills - $103.23
- 270 pills - $148.94
- 360 pills - $194.66
Torsemide 10mg
- 60 pills - $29.14
- 90 pills - $36.02
- 120 pills - $42.90
- 180 pills - $56.65
- 270 pills - $77.29
- 360 pills - $97.92
Torsemide dosages: 20 mg, 10 mg
Torsemide packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
Only $0.29 per item
In stock: 556
Description
Because renal excretion is the primary route for the elimination of sugammadex and the rocuronium-sugammadex complex blood pressure medication diuretic 10 mg torsemide order with mastercard, studies on elimination by dialysis have considerable relevance in clinical practice. In a small subset of patients with severe renal impairment, an investigation on dialysis showed that the clearance of sugammadex and rocuronium in blood was 78 and 89 mL/min, respectively. Therefore hemodialysis using a high-flux dialysis method is effective in removing sugammadex and the sugammadex-rocuronium complex in patients with severe renal impairment. Sugammadex allows a profound neuromuscular blockade to continue until the end of surgery. In clinical practice and during an unexpected difficult airway (cannot intubate, cannot ventilate scenario), a rocuronium neuromuscular blockade may be reversed by sugammadex immediately in order to restore spontaneous ventilation. When sugammadex was compared with neostigmine or edrophonium, the time course of neuromuscular recovery was markedly different. A randomized trial compared the efficacy of sugammadex reversal of a rocuronium (0. Rapid sequence induction and intubation with rocuronium-sugammadex compared with succinylcholine. Reversal of profound rocuronium-induced blockade with sugammadex: a randomized comparison with neostigmine. The use of sugammadex in pediatric patients was examined in a study enrolling 8 infants (28 days to 23 months), 24 children (2-11 years), and 31 adolescents (1217 years). Residual neuromuscular blockade or recurarization was not observed, and no side effects were reported. In a more recent case report, sugammadex was used successfully in reversing a vecuronium-induced neuromuscular blockade in a 7-month-old infant. Reversal of neuromuscular blockade by sugammadex has been assessed in older patients. One hundred and fifty patients were divided into three groups; an adult group (1864 years old), an older adult group (6575 years old), and an oldest adult group (75 years or older). Multicenter, parallel-group, comparative trial evaluating the efficacy and safety of sugammadex in patients with end-stage renal failure or normal renal function. In general, a prolonged circulation time secondary to a reduced cardiac output in older patients was anticipated to result in a longer recovery time from neuromuscular blockade after administration of sugammadex. Patients with a history of pulmonary disease have an increased risk of postoperative pulmonary complications such as pneumonia, respiratory failure, and exacerbation of the underlying pulmonary disease. As in other adult patient groups, reversal of a rocuronium-induced neuromuscular blockade was rapid, and there were no signs of residual neuromuscular blockade or recurarization. Both patients were asthmatic, and there was no evidence that these symptoms were related to sugammadex.
Syndromes
- If there is grimacing, the infant scores 1 for reflex irritability.
- Not urinated for 8 or more hours
- After surgery
- May occur on awakening
- Artificial heart valve
- Fluid or swelling in the sac around the heart
- Bronchopulmonary dysplasia
Physiological characterization of the R1086H mutation further demonstrated that sensitivity of RyR1 activity was significantly enhanced by membrane depolarization or by pharmacologic activators of RyR1 blood pressure medication verapamil generic torsemide 20 mg on line. In murine studies, muscle fibers from Het R174W animals verify the increased sensitivity of Ca2+ release to caffeine and halothane compared with myotubes expressing wild type CaV1. Dantrolene sodium is a hydantoin derivative (1-[5-(4-nitrophenyl)-2-furanyl]methylene] imino]-2,4-imidazolidinedione) that does not block neuromuscular transmission, but causes muscle weakness by direct muscular action. Paul-Pletzer and associates demonstrated that [3H]azidodantrolene specifically labels the amino terminus of RyR1 defined by the 1400-amino acid residue N-terminal calpain digestion fragment of RyR1. Hence for practical reasons, the RyR1 gene remains the primary target for current clinical genetic analysis. These physical links transmit essential signals across the narrow gap of the triadic junction that activate the RyR1 and release Ca2+ from the sarcoplasmic reticulum. It does appear that some mutations are clustered in a given region of the world, but the distribution and frequency appear to be somewhat population specific. In the United Kingdom, 69 RyR1 mutations have been discovered, 25 of which are found only in a single family. Because genetic screening in European and North American studies has predominantly targeted only regions 1 and 2 of the original hot spots in the gene, the absence of RyR1 mutations in some of the screened population could be explained by RyR1 mutations located outside these two regions or by involvement of other genes. The lowest concentration of caffeine which produces a sustained increase of at least 0. Then, the halothane threshold is obtained using the same method by exposing the muscle to halothane concentrations of 0. The dynamic halothane test is performed with the muscle stretched at a constant rate of 4 mm/min to achieve a force of approximately 3 g and held at the new length for 1 min for a 3 min exposure to halothane. Optional tests include exposure of muscle to a combination of both 1% halothane and incremental caffeine concentrations, and to 2% v/v halothane alone. They also reported that the occurrence was more frequent in young males (75%) (median age of 22. A second possibility is variable penetrance with possible allelic silencing,127 and a third is that individuals with discordance have mutations in other unknown genes or modifier genes that affect the function of RyR1 and its phenotypic penetrance. Thus onset of the syndrome in humans is extremely variable both in initial symptoms and in the time of onset of the syndrome. Its onset is so variable that making the diagnosis in the setting of a clinical anesthetic can be quite difficult. Rigidity after induction with thiopental and succinylcholine, but successful intubation, followed rapidly by the symptoms listed after scenario 2. It can be delayed for several reasons and may not be overt until the patient is in the recovery room. Stresses associated with these episodes include exercise and environmental exposure to volatile nonanesthetic vapors.
Specifications/Details
Of course heart attack demi lovato chords buy torsemide 20 mg low cost, selecting target concentrations and different times of rate adjustment is possible, depending on the clinical circumstances and an assessment of how accurately the intravenous drug needs to be titrated. Infusion Rates to Maintain Stable Plasma Concentrations 5 4 Fentanyl (ng/mL) 3 2 1 Suggested initial target 6. The diagonal lines show the infusion rates at different times required to maintain the desired concentration selected on the y axis. Although the terminal elimination half-life is often interpreted as a measure of how short- or long-lasting a drug is, the rate at which drug plasma concentration decreases is dependent on both elimination and redistribution of the drug from the central compartment. The contribution of redistribution and elimination toward the rate of decrease in drug concentration varies according to the duration for which the drug has been administered108,109 and also the time since the infusion has stopped, because these processes have different rate constants. In 1985, Schwilden110 developed a mathematic model to relate the time course of offset of action of inhaled anesthetics to the duration of anesthetic drug delivery. Similarly, Fisher and Rosen111 demonstrated how the accumulation of neuromuscular blocking agents in peripheral volumes of distribution results in slowed recovery with increasing duration of administration. They introduced two measures of the time course of recovery, the time for twitch tension to recover from 5% to 25% and the time for twitch tension to recover from 25% to 75%. Since then, the time for the plasma concentration to decrease by 50% from an infusion that maintains a constant concentration. Additionally, sometimes it is the plasma concentration that is of interest, and sometimes it is the effect-site concentration that is of interest. A more general term is the context-sensitive decrement time,112 in which the decrement in concentration is specifically noted, as is the compartment where the decrease is modeled (plasma or effect site). For example, the relationship between infusion duration and the time required for a 70% decrease in fentanyl effect-site concentration is the context-sensitive 70% effect-site decrement time. To determine when an infusion should be terminated (to enable awakening of the patient at the end of surgery), the clinician needs to bear in mind the decrease in concentration necessary for recovery, the duration of the infusion (the context), and the context-sensitive, effect-site decrement time required for the necessary decrease. Context-sensitive decrement times are fundamentally different from the elimination half-life. With monoexponential decay, each 50% decrease in concentration requires the same amount of time, and this time is independent of how the drug is given. In addition, small changes in percent decrement can result in surprisingly large increases in the time required. Context-sensitive decrement times are based on the assumption that plasma or the effect site is maintained at a constant concentration. Such is rarely the case clinically, but the maintenance of constant concentrations is a necessary assumption to provide a unique mathematic solution to the time required for a given percent decrement in plasma or effect-site concentration.
Sodium Borate (Boron). Torsemide.
- How does Boron work?
- What is Boron?
- Body building.
- Vaginal infections. The most common form of boron called boric acid is applied vaginally for these infections.
- Bone loss (osteoporosis), improving thinking and coordination in older people, and increasing testosterone.
- Are there safety concerns?
- Preventing boron deficiency.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96861
Related Products
Usage: q.h.
Additional information:
Tags: buy torsemide 10 mg lowest price, 10 mg torsemide purchase visa, cheap torsemide 10 mg with visa, purchase 10 mg torsemide with amex
8 of 10
Votes: 108 votes
Total customer reviews: 108
Customer Reviews
Brontobb, 58 years: Peritoneal dialysis requires placement of a catheter in the intraabdominal space; this is typically performed laparoscopically, but can be inserted at the bedside if needed. Neuraxial techniques have been successfully used in isolated spina bifida occulta patients, but are not advised in the setting of severe neural tube defects such as diastematomyelia or tethered cord.
Vasco, 28 years: In theory, magnetic nerve stimulation has several advantages over electrical nerve stimulation. Before topical application of local anesthetic to the airway, administration of an anticholinergic agent should be considered to aid in the drying of secretions, which helps improve both the effectiveness of the topical local anesthetic and visualization during laryngoscopy.