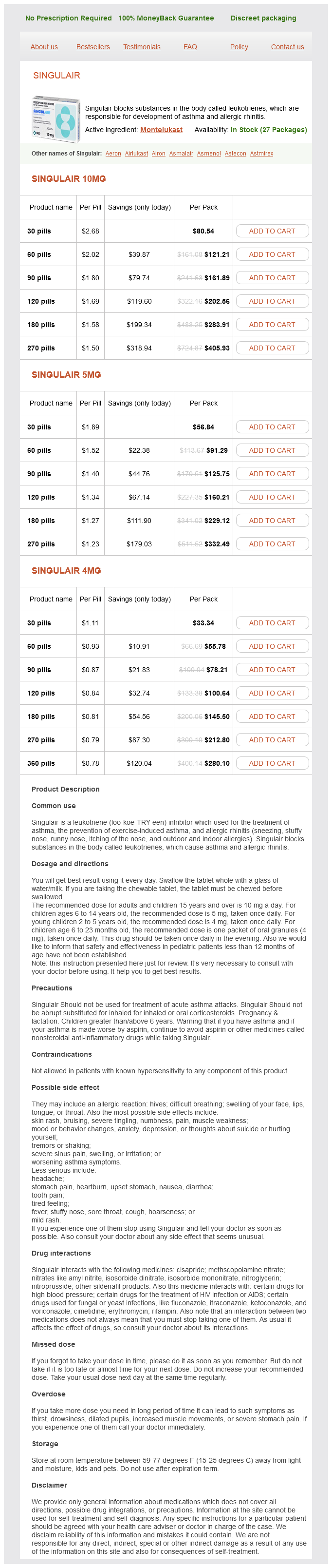
Singulair 10mg
- 30 pills - $80.54
- 60 pills - $121.21
- 90 pills - $161.89
- 120 pills - $202.56
- 180 pills - $283.91
- 270 pills - $405.93
Singulair 5mg
- 30 pills - $56.84
- 60 pills - $91.29
- 90 pills - $125.75
- 120 pills - $160.21
- 180 pills - $229.12
- 270 pills - $332.49
Singulair 4mg
- 30 pills - $33.34
- 60 pills - $55.78
- 90 pills - $78.21
- 120 pills - $100.64
- 180 pills - $145.50
- 270 pills - $212.80
- 360 pills - $280.10
Singulair dosages: 10 mg, 5 mg, 4 mg
Singulair packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
Only $0.83 per item
In stock: 895
Description
This process has potential clinical significance because it may limit the therapeutic response to sympathomimetic agents asthma symptoms 16 month old buy 5 mg singulair with amex. Some mechanisms occur relatively slowly, over the course of hours or days, and these typically involve transcriptional or translational changes in the receptor protein level, or its migration to the cell surface. Rapid modulation of receptor function in desensitized cells may involve critical covalent modification of the receptor, especially by phosphorylation of specific amino acid residues, association of these receptors with other proteins, or changes in their subcellular location. There are two major categories of desensitization of responses mediated by G protein-coupled receptors. Homologous desensitization refers to loss of responsiveness exclusively of the receptors that have been exposed to repeated or sustained activation by an agonist. Heterologous desensitization refers to the process by which desensitization of one receptor by its agonists also results in desensitization of another receptor that has not been directly activated by the agonist in question. Specific adrenoceptors become substrates for these kinases only when they are bound to an agonist. This mechanism is an example of homologous desensitization because it specifically involves only agonist-occupied receptors. Phosphorylation of these receptors enhances their affinity for arrestins, a family of four proteins, of which the two nonvisual arrestin subtypes are widely expressed. In addition to desensitizing agonist responses mediated by G proteins, arrestins can trigger G protein-independent signaling pathways. Recognition that G protein-coupled receptors can signal through both G protein-coupled and G protein-independent pathways has raised the concept of developing biased agonists that selectively activate these arrestin-coupled signaling pathways (see Box: Therapeutic Potential of Biased Agonists at Beta Receptors). For the 2 receptor, protein kinase A phosphorylation occurs on serine residues in the third cytoplasmic loop of the receptor. Similarly, activation of protein kinase C by Gq-coupled receptors may lead to phosphorylation of this class of G protein-coupled receptors. This second-messenger feedback mechanism has been termed heterologous desensitization because activated protein kinase A or protein kinase C may phosphorylate any structurally similar receptor with the appropriate consensus sites for phosphorylation by these enzymes. Beta1 receptors are also coupled through G protein-independent signaling pathways involving -arrestin, which are thought to be cardioprotective. A "biased" agonist could potentially activate only the cardioprotective, -arrestinmediated signaling (and not the G protein-coupledmediated signals that lead to greater cardiac workload). Such a biased agonist would be of great therapeutic potential in situations such as myocardial infarction or heart failure. Biased agonists potent enough to reach this therapeutic goal have not yet been developed. Adrenoceptor Polymorphisms Since elucidation of the sequences of the genes encoding the 1, 2, and subtypes of adrenoceptors, it has become clear that there are relatively common genetic polymorphisms for many of these receptor subtypes in humans.
Syndromes
- Itching eyes
- Barium enema
- Low-fat diet
- Osteomalacia
- Problems breathing
- Opium
- Blood flow in the abdomen
- As a screening test for women over age 30
- Feeling ashamed, guilty, or like a burden to others
As a result of its strong antimuscarinic actions asthma treatment xopenex generic 4 mg singulair visa, cyclobenzaprine may cause significant sedation, as well as confusion and transient visual hallucinations. The dosage of cyclobenzaprine for acute injury-related muscle spasm is 2040 mg/d orally in divided doses. Llauradó S et al: Sugammadex ideal body weight dose adjusted by level of neuromuscular blockade in laparoscopic bariatric surgery. Part I: Definitions, incidence, and adverse physiologic effects of residual neuromuscular block. Naguib M et al: Advances in neurobiology of the neuromuscular junction: Implications for the anesthesiologist. Metaxalone Generic, Skelaxin Methocarbamol Generic, Robaxin Orphenadrine Generic, Norflex, others Riluzole Generic, Rilutek Note: this drug is labeled only for use in amyotrophic lateral sclerosis. Lee C et al: Reversal of profound neuromuscular block by sugammadex administered three minutes after rocuronium. Draulans N et al: Intrathecal baclofen in multiple sclerosis and spinal cord injury: Complications and long-term dosage evolution. Frydrych V, Oderda G: Skeletal muscle relaxants drug class review: University of Utah College of Pharmacy. Krause T et al: Dantrolene-A review of its pharmacology, therapeutic use and new developments. To avoid possible aspiration at the time of intubation, a very rapid-acting muscle relaxant should be used so the airway can be secured with an endotracheal tube. Usually, succinylcholine would be the agent of choice in this case; however, the patient has a ruptured (open) globe. Succinylcholine is contraindicated in patients with an open globe because it raises intraocular pressure and could possibly result in extrusion of aqueous or vitreous humor. Therefore, a rapid sequence intubation should be performed with high-dose (up to 1. At this dose, rocuronium has a very rapid onset, which approaches but does not quite equal that of succinylcholine. In the case vignette, you are unable to intubate the patient and may be unable to mask ventilate the patient. Since a large dose of rocuronium was just given, a dose of 16 mg/kg of sugammadex needs to be given to rapidly and completely reverse the effects of the neuromuscular blocking agent and allow return of spontaneous ventilation. In order to proceed with surgery, another technique (such as an awake fiberoptic-assisted intubation) should be used to secure the airway. He has developed a stooped posture, drags his left leg when walking, and is unsteady on turning. He remains independent in all activities of daily living, but he has become more forgetful and occasionally sees his long-deceased father in his bedroom.
Specifications/Details
A well-documented mechanism involves the 2 receptor located on noradrenergic nerve terminals asthmatic bronchitis deaths 4 mg singulair buy with amex. This receptor is activated by norepinephrine and similar molecules; activation diminishes further release of norepinephrine from these nerve endings (Table 64). The mechanism of this G protein mediated effect involves inhibition of the inward calcium current that causes vesicular fusion and transmitter release. Conversely, a presynaptic receptor appears to facilitate the release of norepinephrine from some adrenergic neurons. Presynaptic receptors that respond to the primary transmitter substance released by the nerve ending are called autoreceptors. Autoreceptors are usually inhibitory, but in addition to the excitatory receptors on noradrenergic fibers, many cholinergic fibers, especially somatic motor fibers, have excitatory nicotinic autoreceptors. Control of transmitter release is not limited to modulation by the transmitter itself. Nerve terminals also carry regulatory receptors that respond to many other substances. Such heteroreceptors may be activated by substances released from other nerve terminals that synapse with the nerve ending. For example, some vagal fibers in the myocardium synapse on sympathetic noradrenergic nerve terminals and inhibit norepinephrine release. Alternatively, the ligands for these receptors may diffuse to the receptors from the blood or from nearby tissues. Some of the transmitters and receptors identified to date are listed in Table 64. Vascular smooth muscle in skeletal muscle has sympathetic cholinergic dilator fibers. Parasympathetic fibers innervate muscarinic receptors in vessels in the viscera and brain, and sympathetic cholinergic fibers innervate skeletal muscle blood vessels. The muscarinic receptors in the other vessels of the peripheral circulation are not innervated and respond only to circulating muscarinic agonists. The cholinergic innervation of the rectum and the genitourinary organs may be anatomically sympathetic; see Box: Sympathetic Sacral Outflow. Note that two feedback loops are present: the autonomic nervous system loop and the hormonal loop. The sympathetic nervous system directly influences four major variables: peripheral vascular resistance, heart rate, force, and venous tone. The net feedback effect of each loop is to compensate for changes in arterial blood pressure. Thus, decreased blood pressure due to blood loss would evoke increased sympathetic outflow and renin release.
Euphorbia cyparissias (Cypress Spurge). Singulair.
- What is Cypress Spurge?
- Are there safety concerns?
- Breathing disorders, diarrhea, or skin diseases.
- How does Cypress Spurge work?
- Dosing considerations for Cypress Spurge.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96433
Related Products
Usage: p.r.n.
Additional information:
Tags: purchase 5 mg singulair, discount 10 mg singulair overnight delivery, 10 mg singulair buy fast delivery, 10 mg singulair with visa
8 of 10
Votes: 298 votes
Total customer reviews: 298
Customer Reviews
Peratur, 58 years: Note that some doses of drug A can produce larger effects than any dose of drug B, despite the fact that we describe drug B as pharmacologically more potent. Botulinum toxin has been approved for use in patients who do not tolerate or are refractory to antimuscarinic drugs. Gilles de la Tourette syndrome is characterized by chronic multiple tics; its pharmacologic management is discussed at the end of this chapter. Clozapine is sometimes associated with myocarditis and must be discontinued if myocarditis manifests.
Arakos, 57 years: Treatment for torsades requires recognition of the arrhythmia, withdrawal of any offending agent, correction of hypokalemia, and treatment with maneuvers to increase heart rate (pacing or isoproterenol); intravenous magnesium also appears effective, even in patients with normal magnesium levels. Most experts recommend coronary angiography and revascularization (if not contraindicated) in patients with stable chronic angina refractory to three-drug medical treatment. In general, if plasma levels above 9 mcg/mL are avoided, lidocaine is well tolerated. It has a bioavailability of about 60%, is extensively metabolized, and has an elimination half-life of about 5 hours.
Rhobar, 35 years: They also may be of benefit in treating the hypertriglyceridemia that results from treatment with antiviral protease inhibitors. Varenicline also has antagonist properties that persist because of its long half-life and high affinity for the receptor; this prevents the stimulant effect of nicotine at presynaptic 42 receptors that causes release of dopamine. In marked contrast to the benzodiazepines, the anxiolytic effects of buspirone may take 34 weeks to become established, making the drug unsuitable for management of acute anxiety states. Tapentadol carries risk for seizures in patients with seizure disorders and for the development of serotonin syndrome.