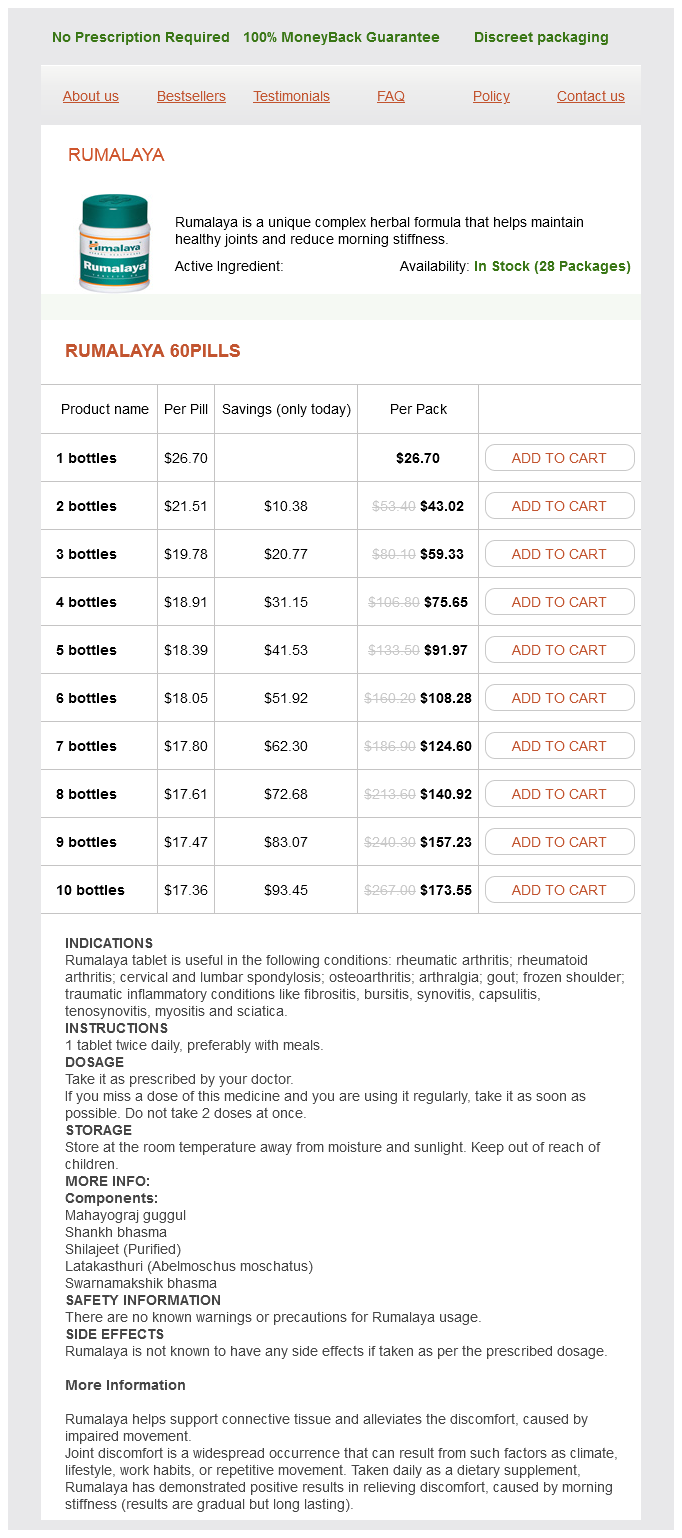
Rumalaya 60pills
- 1 bottles - $26.70
- 2 bottles - $43.02
- 3 bottles - $59.33
- 4 bottles - $75.65
- 5 bottles - $91.97
- 6 bottles - $108.28
- 7 bottles - $124.60
- 8 bottles - $140.92
- 9 bottles - $157.23
- 10 bottles - $173.55
Rumalaya dosages: 60 pills
Rumalaya packs: 1 bottles, 2 bottles, 3 bottles, 4 bottles, 5 bottles, 6 bottles, 7 bottles, 8 bottles, 9 bottles, 10 bottles
Only $18.44 per item
In stock: 769
Description
Under normal circumstances medicine 1900s spruce cough balsam fir buy rumalaya 60 pills line, inflation of the lung is maintained because although the pressure inside (alveolar pressure) is zero, the outside pressure. The inward force is the "elastic recoil" of the lung and emanates from the elastic lung tissue fibers, contractile airway smooth muscle, and alveolar surface tension. The outward force is developed by passive recoil from the ribs, joints, and muscles of the chest wall. First, inflating an already opened (inflated) lung is easier than when the lung is already deflated. This is because complete collapse results in liquid-only surfaces interfacing in alveoli (high surface tension), whereas alveoli in partially inflated lung have air-liquid interfaces (lower surface tension). Second, although perfusion in the lung is phasic, the frequency is rapid and the oscillations in flow are low, resulting in nearly continuous flow. Ventilation is different: the frequency is far slower and the size of the oscillations far larger. Chest wall mechanics can be measured only if complete relaxation of the respiratory muscles can be achieved26; however, during mechanical ventilation the respiratory muscles can be completely relaxed. Values of chest wall compliance are about the same as that of the lung and are reduced with obesity, chest wall edema, pleural effusions, and diseases of the costovertebral joints. The major component of resistance is the resistance exerted by the airways (large and small), and a minor component is the sliding of lung and the chest wall tissue elements during inspiration (and expiration). Resistance (R) is calculated as driving pressure (P) divided by the resultant gas flow (F): R = P/F the value of airway resistance is approximately 1 cm H2O/L/sec, and is higher in obstructive lung disease. Two factors explain why most (approximately 80%) of the impedance to gas flow occurs in the large airways. Second, in tubes that are large, irregular or branched, the flow is often turbulent, not laminar. When flow is laminar: F(lam) = P/R In contrast, when flow is turbulent: F(turb) = P/R2 Therefore, for a given radius, far more pressure is required to achieve comparable flow where flow is turbulent; thus, the effort required is greater and if prolonged or severe, respiratory failure is more likely. First, resistance lessens as lung volume increases; this is intuitive as increasing volume (positive pressure or spontaneous breathing) stretches the diameter of the airways; because this is the key determinant of resistance, the resistance falls to a small extent. In fibrosis, the slope of the curve is flatter, reflecting considerable increases in pressure variation and in respiratory work. In asthma or bronchitis, there is a parallel (upward) shift of the pressure-volume curve, indicating an increase in lung volume but no change in compliance. In emphysema, the slope of the curve is steeper, reflecting tissue loss and possible increased compliance. However, in emphysema, asthma, or bronchitis, the airway resistance is increased; this increases work of breathing and overrides any benefit from increased compliance. This results in different positions on the pressure volume curve of the upper (flatter, less compliant) versus lower (steeper, more compliant) lung regions. Schematic drawing of airflow resistance against lung volume at different flow rates.
Syndromes
- Seizures
- Astrovirus
- A few days before surgery, you will be given a bowel prep that includes drinking fluids and taking laxatives and enemas. This is done to make sure that the colon is free of any stool.
- You may have an object in your eye.
- Medications
- Malabsorption
- Breathing problems
- To diagnose heart rhythm problems
These devices should be located at "every anesthetizing location medicine tramadol rumalaya 60 pills order with mastercard," and the guideline further recommends that they be checked for proper function. The recommendation also states that the auxiliary oxygen source should be separate from the machine and its pipeline supply, "specifically an oxygen cylinder. Item 2: Verify Patient Suction Is Adequate to Clear the Airway Frequency: Before each use Responsible parties: Provider and technician "Safe anesthetic care requires the immediate availability of suction to clear the airway if needed. However, the process of checking alarm thresholds, and possibly resetting them, can be tedious. Monitor alarm settings may possibly vary within individual facilities as a result of provider manipulation of alarms for case requirements, a lack of standard default settings, and failure to reset alarm limits routinely. Departmental alarm default settings can be established and programmed into anesthesia workstation monitors. Alarm limit settings also include anesthesia machine alarms such as volume, pressure, and inspired oxygen concentration limits. The practitioner should ensure that critical alarm limits are set to values that permit these alarms to do what they were intended to do. Desflurane vaporizers require electrical power and recommendations for checking power to these vaporizers should also be followed. The ability to conform to these standards should be confirmed for every anesthetic. Alarm limit values are easy to adjust, although this process can be time consuming during routine preuse checkout. Safe default values can be established locally and set by trained technicians, to help keep limits consistent. Chapter 29: Inhaled Anesthetics: Delivery Systems 807 Here, anesthesia technicians can improve the quality of the preuse checkout by checking the function of standard monitors and confirming that critical alarm thresholds are set to established default values. The acceptable pressure depends on the intended use, the design of the anesthesia delivery system and the availability of piped oxygen. Some newer machines may also have a tank gauge located on the back of the machine. Therefore the pressure in the piped gas supply should be checked at least once daily. As discussed earlier, if the tank is to be used in the setting of a suspected oxygen pipeline contamination, the pipeline supply must be disconnected from the machine for tank gas to flow into the gas supply system. In that case, the maximum duration of oxygen supply can be obtained from an oxygen cylinder if it is used only to provide fresh gas to the patient in conjunction with manual or spontaneous ventilation. Mechanical ventilators will consume the oxygen supply if pneumatically powered ventilators that require oxygen to power the ventilator are used. Electrically-powered ventilators do not consume oxygen so that the duration of Normal pipeline pressures in the United States for common gases (oxygen, air, nitrous oxide) are 50 to 55 psig.
Specifications/Details
The muscarinic (M3) receptors are located postsynaptically on airway smooth muscle symptoms weight loss rumalaya 60 pills purchase on line. Dose response to mivacurium in patients under nitrous oxideoxygenopioid anesthesia. Several case reports described the occurrence of severe bradycardia and even asystole after vecuronium or atracurium administration. Subsequent studies indicated that administration of vecuronium or atracurium alone does not cause bradycardia. Thus, the moderate vagolytic effect of pancuronium is often used to counteract opioid-induced bradycardia (see also Chapter 31). The muscarinic cholinergic system plays an important role in regulating airway function. Five muscarinic receptors have been cloned,197 three of which (M1 to M3) exist in the airways. Support for this concept is provided by the finding that prior administration of atropine attenuates or eliminates the cardiovascular effects of pancuronium. Succinylcholine and dTc actually reduce the incidence of epinephrine-induced dysrhythmias. The affinity of the compound rapacuronium to block M2 receptors is 15 times higher than its affinity to block M3 receptors. Anaphylactoid reactions are not immune mediated and represent exaggerated pharmacologic responses in very rare and very sensitive individuals. Watkins stated, "The much higher incidence of rocuronium reactions reported in France is currently inexplicable and is likely to remain so if investigators continue to seek a purely antibody-mediated response as an explanation of all anaphylactoid reaction presentations. More recent publications have highlighted the need for standardization of diagnostic procedures of anaphylactic reactions. Biochemical tests should be performed rapidly after occurrence of an anaphylactic reaction. An early increase in plasma histamine is observed 60 to 90 minutes after anaphylactic reactions. Serum tryptase concentrations typically reach a peak between 15 and 120 minutes, depending on the severity of the reaction. For instance, Laxenaire used a 1:10 dilution of rocuronium for interdermal skin testing,212 whereas Rose and Fisher used a 1:1000 dilution. In vitro physical or chemical incompatibilities are not considered drug interactions. Further, inhibition of butyrylcholinesterase by pancuronium results in decreased plasma clearance of mivacurium and marked potentiation of the neuromuscular blockade. After the administration of pancuronium, recovery from the first two maintenance doses of vecuronium is reportedly prolonged, although this effect becomes negligible by the third dose. The apparent prolongation of action of the first maintenance dose of mivacurium administered after atracurium,218 and of those reported with vecuronium after pancuronium,222,223 is not related to synergism. Combinations of atracurium and mivacurium218 and of vecuronium and pancuronium98 are simply additive.
European Hellebore (White Hellebore). Rumalaya.
- How does White Hellebore work?
- What is White Hellebore?
- Dosing considerations for White Hellebore.
- Treating cholera, gout, hypertension, and herpes (cold sores).
- Are there safety concerns?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96361
Related Products
Usage: b.i.d.
Additional information:
Tags: rumalaya 60 pills low price, rumalaya 60 pills on-line, generic rumalaya 60 pills with mastercard, rumalaya 60 pills buy on-line
8 of 10
Votes: 307 votes
Total customer reviews: 307
Customer Reviews
Kor-Shach, 50 years: This section focuses on body habitus and age, both known to influence the pharmacology of many anesthetic drugs and both of which serve as excellent examples of altered pharmacokinetics and pharmacodynamics. Coronary collateral perfusion was unchanged during isoflurane or halothane anesthesia in dogs at a mean arterial pressure of 50 mm Hg. Edrophonium-atropine mixtures induced small increases in heart rate, whereas edrophonium-glycopyrrolate mixtures caused decreases in heart rate and occasionally severe bradycardia. Although clinical studies indicate that sevoflurane is most likely safe even in patients with preexisting renal dysfunction, the drug should be administered in accordance with the approved package labeling guidelines.
Dawson, 26 years: In contrast, investigators reported that opioids also stimulate Ca2+ influx in neuronal cultured cells. Therefore, its clinical utility is rather limited considering newer anticonvulsants are available with fewer and less severe side effects. The pressure-volume characteristics of this bag are such that it inflates to a maximal pressure and then slightly decreases to a plateau as it continues to fill even to high volumes. Most vagal fibers do not synapse until they arrive at small ganglia on and about the thoracic and abdominal viscera.