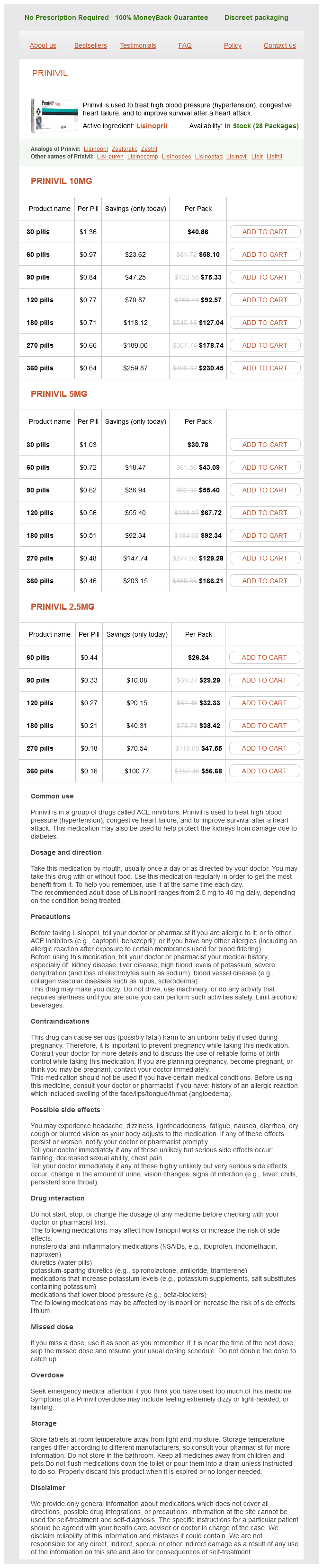
Prinivil 10mg
- 30 pills - $40.86
- 60 pills - $58.10
- 90 pills - $75.33
- 120 pills - $92.57
- 180 pills - $127.04
- 270 pills - $178.74
- 360 pills - $230.45
Prinivil 5mg
- 30 pills - $30.78
- 60 pills - $43.09
- 90 pills - $55.40
- 120 pills - $67.72
- 180 pills - $92.34
- 270 pills - $129.28
- 360 pills - $166.21
Prinivil 2.5mg
- 60 pills - $26.24
- 90 pills - $29.29
- 120 pills - $32.33
- 180 pills - $38.42
- 270 pills - $47.55
- 360 pills - $56.68
Prinivil dosages: 10 mg, 5 mg, 2.5 mg
Prinivil packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
Only $0.17 per item
In stock: 830
Description
Patients can be divided into the following three groups for application of surgical procedures: 1 hypertension lifestyle modification prinivil 10 mg without prescription. Those with retraction and significant proptosis the procedures needed for correction of lower lid retraction with prominent eyes include canthal anchoring and release procedures in the lower lid (see Chapter 8). Because tightening the lower lid in the presence of exophthalmos can produce a downward clotheslining of the lid, compensatory procedures may be needed. B, the same patient 4 months after conventional blepharoplasty and a modified midface lift. Fat transfer to the malar area is combined with a vertical cheek lift to produce more fullness in the malar area to minimize eye prominence. Because of the clotheslining tendency with tightening of the lower lid, the need for spacers and release procedures may be necessary in these patients. Principle of clotheslining: In a prominent eye, tightening the lid can cause downsliding of the lower lid. In some patients, spacers are placed transconjunctivally when external skin redraping is not needed. If blepharoplasty combined with midface skin redraping and fat transfer is used, an external incision for spacer placement may be more appropriate. A spacer can be inserted in the posterior lamella of the lid either transconjunctivally or transcutaneously. Technique With the external approach, a subciliary incision is made to elevate a skin-muscle septal flap. The midface lift is performed (see Chapter 8) and combined with fat transfer and canthal anchoring. With significant lid retraction, scleral show may still be present after canthal anchoring. In some cases, recession of the capsulopalpebral fascia may adequately restore the lower lid position. B, Lower lid retractors (capsulopalpebral fascia and inferior tarsal muscle) have been peeled away from the underlying conjunctiva. C, A spacer is then inserted between the inferior tarsal edge and recessed retractors (ear cartilage in this case). D, the external skin-muscle flap is sutured back into position after blepharoplasty. B, the patient is seen after spacers were inserted into both lower lids and the right upper lid.
Syndromes
- Loss of appetite and weight loss
- Pain with intercourse or ejaculation
- Scalp defects (missing skin)
- Lymph nodes
- Back pain
- You have palpitations with chest pain or other symptoms
- Your doctor or nurse will tell you when to arrive at the hospital. Be sure to arrive on time.
Restorative proctocolectomy with ileoanal pouch is the most recently 130 devised procedure for ulcerative colitis blood pressure chart time of day order prinivil 10 mg without prescription, and avoids the need for permanent © 2016 Health Press Ltd. It is now the favored operation in younger patients (particularly those younger than 60 years) in whom preoperative confirmation of normal anal sphincter function minimizes the risk of postoperative incontinence of liquid pouch contents. Although proctocolectomy and ileostomy have the lowest morbidity and mortality of operations for ulcerative colitis, ileostomy incurs a readmission rate of about 50% in 10 years. Because of its effects on body image, hygiene, and social and sexual function, a small minority of patients find an ileostomy impossible to adapt to psychologically. The diagnosis of pouchitis is made in patients with worsening diarrhea and/or bleeding, endoscopic signs of inflammation and histological evidence of acute inflammation with neutrophil infiltration and ulceration. In some cases it is caused by ischemia which should be suspected if pouchitis is asymmetrical. In most cases it represents a recurrent ulcerative colitis-like condition in the pouch with genetic, immunologic and microbial factors contributing to the pathogenesis. The importance of host susceptibility is shown by the fact that patients undergoing the same operation for familial polyposis coli seldom develop pouchitis. About 40% of patients will have at least one episode in the first 10 years after pouch construction. Therapeutic options include metronidazole (10 mg/kg in divided daily doses) for at least 10 days, ciprofloxacin alone or in combination with metronidazole, and topical or 132 oral corticosteroids or aminosalicylates (as for ulcerative colitis; see Chapter 7). Probiotic treatment, particularly after antibiotics, has been reported to be effective, but the results in different centers are variable. A minority of patients with refractory pouchitis require pouch resection and a permanent ileostomy. Surgery is indicated primarily for disease refractory to medical and/or nutritional therapy, or for complications Table 9. Ileocecal disease is excised with a limited right hemicolectomy, in which the ileum is anastomosed to the ascending colon, with removal of involved ileum, cecum and appendix. Ileoanal pouch creation is contraindicated by a high frequency of anastomotic leaks and sepsis, which necessitate its removal. Even in patients with rectal sparing, the recurrence rate is much higher with colectomy and ileorectal anastomosis than with proctocolectomy and ileostomy, making the latter preferable. In rare patients with localized colonic disease, segmental resection (unlike in ulcerative colitis) is a reasonable option. Abscesses require drainage, and complex chronic fistulas may need insertion of loose (seton) sutures to facilitate continued drainage. Defunctioning ileostomy or colostomy may allow healing of severe perianal disease by diverting the fecal stream, but recurrence after closure of the stoma is common. In about 70% of patients, colonoscopy shows recurrent aphthoid ulceration, usually immediately proximal to the anastomosis, 1 year after right hemicolectomy. Postoperative treatment with oral metronidazole for 3 months reduces the endoscopic recurrence rate at 1 year, but the effect of such therapy on the symptomatic recurrence rate of 50% at 5 years and the rate of need for repeat surgery of 50% at 10 years is not clear (see Chapter 8).
Specifications/Details
D blood pressure 80 60 discount prinivil 10 mg online, Low power photomicrograph of curetted material from C shows thickened septum of aneurysmal bone cyst with focus of chondroid matrix and sheets of chondroblasts. Personal Comments A useful radiologic feature of aneurysmal bone cyst, the "finger-in-the-balloon" sign, has been observed by Dr. This is the preservation of a cortical bone cuff that penetrates for a short distance into the expanded area of destructive blowout. This sign is not present in telangiectatic osteosarcoma or other aggressive malignant tumors of bone. The most frequent histologic obstacle in the recognition of aneurysmal bone cyst is the presence of significant amounts of reactive bone and osteoid within the septa and even in solid areas of the lesion. They are usually oriented along the septa, unlike the random orientation of osteoid and tumor bone trabeculae of osteosarcomas. Microscopic features of an aneurysmal bone cysts are often combined with those of giant cell reparative granuloma, especially in lesions found in the short tubular bones of the hands and feet and in vertebral lesions. The composite nature of these lesions suggests that aneurysmal bone cyst and giant cell reparative granuloma may represent closely related but distinct reactions to intraosseous hemorrhage after trauma. Giant cell tumor Chondroblastoma Osteoblastoma Nonossifying fibroma Fibrous dysplasia Giant cell reparative granuloma Chondromyxoid fibroma Fibrous histiocytoma Solitary bone cyst condition for the development of secondary aneurysmal bone cyst in the small bones of the hands and feet and in the mandible. Fibrous dysplasia should be considered in reference to lesions located in the shafts of long bones of the extremities, in the ribs, and in the craniofacial region. In the metaphyseal parts of the long tubular bones, especially in a lower extremity, lesions such as nonossifying fibroma and, less frequently, chondromyxoid fibroma should be considered. The most frequent underlying condition for secondary aneurysmal bone cyst of the vertebral column is osteoblastoma. Osteoblastoma should also be anticipated in sites such as the mandible and the maxilla. The most frequent underlying conditions for secondary aneurysmal bone cyst are listed in Table 15-1. It must be remembered that aneurysmal bone cyst is rarely superimposed on primary or metastatic malignant tumors. Therefore it can be seen even in such conditions as vascular cartilaginous hamartoma. Differential Diagnosis Differential diagnosis of a secondary aneurysmal bone cyst is similar to that of a primary aneurysmal bone cyst. Treatment and Behavior the treatment and behavior of secondary and primary aneurysmal bone cysts are similar. For example, the patient with an aneurysmal bone cyst Soft Tissue Aneurysmal Bone Cyst Aneurysmal bone cysts very rarely arise in extraosseous sites, including the somatic soft tissue of the extremities, most often in the thigh and shoulder regions. However, the term unicameral is misleading because some of these lesions may consist of several multilocular cavities. Definition Solitary bone cyst is typically a unilocular cystic lesion that does not have a lining and is filled with serous fluid. It arises most frequently in the metaphyseal portion of the major long bones, such as the humerus or femur, in skeletally immature patients.
Chicory. Prinivil.
- Dosing considerations for Chicory.
- How does Chicory work?
- Constipation, liver and gallbladder disorders, cancer, skin inflammation, loss of appetite, upset stomach, and other conditions.
- What is Chicory?
- Are there safety concerns?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96136
Related Products
Usage: p.o.
Additional information:
Tags: buy 10 mg prinivil overnight delivery, cheap prinivil 5 mg buy line, buy cheap prinivil 10 mg on line, order prinivil 2.5 mg online
10 of 10
Votes: 57 votes
Total customer reviews: 57
Customer Reviews
Lares, 23 years: A and B, Two examples of bony and cartilaginous exostotic lesions of phalanx and metacarpal bone in a 38-year-old man and a 61-yearold woman, respectively.
Rathgar, 38 years: When injecting the corrugators, this effect can be reduced by also injecting a smaller amount of botulinum toxin into the frontalis muscle to reduce glabellar frowning without causing a widening of the brow spacing.
Ronar, 22 years: Causes of Horner syndrome are multiple, and the patient should be evaluated by a neurologist if the cause has not been previously diagnosed.
Renwik, 35 years: The ideal position of the lateral canthus for ideal function varies from patient to patient and is dependent on the mechanics of both the eyelids and the downward force on the lid by the globe, which is directly proportional to the prominence of the globe.
Irhabar, 55 years: This term encompasses previously used designations such as malignant schwannoma, neurofibrosarcoma, and neurogenic sarcoma.
Marus, 42 years: Affected individuals develop hemangioblastomas in the central nervous system, clear cell carcinomas of the kidney, pheochromocytomas of the adrenal gland, extraadrenal paragangliomas, endolymphatic sac tumors, pancreatic microcystic adenomas, and pancreatic neuroendocrine tumors.
Roland, 48 years: Lagier R, Mbakop A, Bigler A: Osteopoikilosis: a radiological and pathological study.