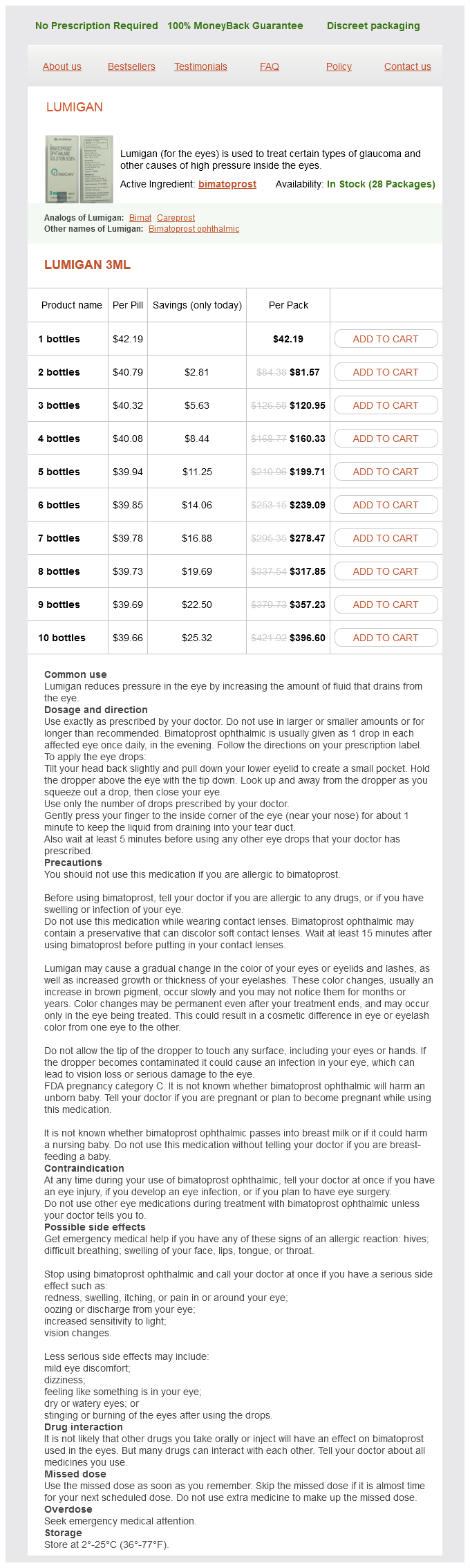
Lumigan 3ml
- 1 bottles - $42.19
- 2 bottles - $81.57
- 3 bottles - $120.95
- 4 bottles - $160.33
- 5 bottles - $199.71
- 6 bottles - $239.09
- 7 bottles - $278.47
- 8 bottles - $317.85
- 9 bottles - $357.23
- 10 bottles - $396.60
Lumigan dosages: 3 ml
Lumigan packs: 1 bottles, 2 bottles, 3 bottles, 4 bottles, 5 bottles, 6 bottles, 7 bottles, 8 bottles, 9 bottles, 10 bottles
Only $42.14 per item
In stock: 797
Description
They are not strictly medical terms but are also literary; philosophic medicine synonym discount 3 ml lumigan with visa, and psychologic ones. William James remarked that everyone knows what con sciousness is until he attempts to define it. For this reason, they use the term consciousness in its broadest operational meaning-namely, the state of awareness of self and environment, and responsive ness to external stimulation and inner need. This narrow definition has an advantage in that unconsciousness has the opposite meaning: a state of unawareness of self and environment or a suspension of those mental activities by which people are made aware of themselves and their environment, coupled always with a diminished respon siveness to environmental stimuli. Arousal, or the level of consciousness, refers to the appearance of being awake as displayed by the facial muscles, eye opening, fixity of gaze, and body posture, i. A clear distinction is made in medicine between the level of consciousness and the content of consciousness, the latter reflecting the quality and coher ence of thought and behavior. For neurological purposes, the loss of normal arousal is by far the more important and dramatic aspect of disordered consciousness and the one identified by laypersons and physicians as being the central feature of coma. Much more could be said about the history of our ideas concerning consciousness, and the theoretical problems with regard to its definition. There has been an ongoing polemic among philosophers of mind as to whether it will ever be possible to understand mind and consciousness in terms of reductionist physical entities, such as cellular and molecular neural systems. This normal state may fluctu ate during the day from one of keen alertness or deep concentration with a marked constriction of the field of attention to one of mild general inattentiveness, but even in the latter circumstances, the normal individual can be brought immediately to a state of full alertness and function. The term confusion lacks preciSion, but in general it denotes an inability to think with customary speed, clarity, and coherence. Almost all states of confusion are marked by some degree of inattentiveness and disorientation. In this condition the patient does not take into account all elements of his immediate environment. This state also implies a degree of imperceptiveness and distractibility, referred to traditionally as "clouding of the sensorium. Confusion results most often from a process that influ ences the brain globally, such as a toxic or metabolic distur bance or a dementia. In addition, any condition that causes drowsiness or stupor, including the natural state that comes from sleep deprivation, results in some degradation of mental performance and the emergence of inattentive ness and a state of confusion. In this way, confusion, which exists along the axis of content of consciousness, is linked to alertness and the level of consciousness. A confusional state can also accompany focal cere bral disease in various locations, particularly in the right hemisphere, or result from disorders that disturb mainly language, memory, or visuospatial orientation, but a distinction is made between these isolated disruptions in mental function and the global confusional state. They represent special states that are analyzed differently, mat ters discussed further in Chaps. The patient may even be roughly oriented as to time and place, with only occasional irrelevant remarks betraying a lack of clarity and slowness of thinking. Their responses are inconsis tent, attention span is reduced, and they are unable to stay on one topic, together suggesting a fundamental flaw in attention.
Syndromes
- Decreased consciousness
- Have you breathed in or swallowed any irritating substances?
- Have regular contact with blood at work (such as a health care worker)
- Headaches
- Antibody testing to check for paraneoplastic syndromes
- Muscle ache without an obvious cause, such as exercise or injury
- Bleeding after sex
- CBC with differential
- Toxicology (poison) screening
A loss of proprioception-as occurs in patients with severe large-fiber polyneuropathy medicine reminder app lumigan 3 ml purchase otc, posterior nerve root lesions. After years of training, such patients still have difficulty in initiating gait and in forward propulsion. Purdon Martin illustrated, they hold their hands slightly in front of the body, bend the body and head forward, walk with a wide base and irregular, uneven steps, but still rock the body. If they are tilted to one side, they fail to compensate for their abnormal pos ture. If they fall, they cannot rise without help; they are sometimes unable to crawl or to get into an "all fours" posture. When standing, if instructed to close their eyes, they sway markedly and fall (Romberg sign); this sign is the clearest indication that the origin of the problem is a loss of proprioceptive sensibility. With lesions of the basal ganglia, both in monkeys and in humans, the posture of the body and the postural responses to perturbations in equilibrium are faulty. There is difficulty in taking the first step; once it is taken, and in extreme cases, the body pitches forward and a fall can be prevented only by catch-up stepping (propulsive festination). Similarly, a step backward may induce a series of quickening steps in that direction (retropulsive fesitnation). Corrective righting reflexes are clearly faulty when the patient is pushed off balance (Denny-Brown). These abnormalities are elaborated further on, under "Parkinsonian and Festinating Gait. Slowness of the swing phase and reduction in the amount of time spent with the painful limb in contact with the ground may be clues to recognizing rheumatological and orthopedic causes of a gait disorder. It is good practice to watch patients as they walk into the examining room, when they are apt to walk more naturally than during the performance of commanded tasks. They should be asked to stand with feet together and head erect, with eyes open and then closed. A normal person can stand with feet together and eyes closed while moving the head from side to side, a test that blocks both visual and vestibular cues and induces certain compensatory trunk and leg movements that depend solely on proprioceptive afferent mecha nisms (Ropper). As already mentioned, the Romberg sign-marked swaying or falling with the eyes closed but not with the eyes open-usually indicates a loss of postural sense, not of cerebellar function, although with vestibular or cerebellar disease there may be an exag geration of swaying. Swaying due to of nervousness may be overcome by asking the patient to touch the tip of his nose alternately with the forefinger of one hand and then the other. A tendency to veer to one side, as occurs with unilateral cerebellar or vestibular disease, can be brought out by having the patient walk around a chair. When the affected side is toward the chair, the p atient tends to w alk into it; when it is away from the chair, there is a veering outward in ever-widening circles. More delicate tests of gait are walking a straight line heel to toe ("tandem walking test"), walking back ward, and having the patient arise quickly from a chair, walk briskly, stop and turn suddenly, walk back, and sit down again. Turning the patient three full revolutions with eyes open, first right and then left, each time fol lowed by asking the patient to walk naturally, allows the examiner to stress the vestibular apparatus and to compare the two sides.
Specifications/Details
When left unstimulated medications voltaren 3 ml lumigan purchase otc, these patients quickly drift back into a deep sleep-like state. The eyes move out ward and upward, a feature that is shared with sleep (see further on). Tendon and plantar reflexes, and the breath ing pattern may or may not be altered, depending on how the underlying disease has affected the nervous system. In psychiatry, the term stupor has been used in a second sense-to denote an uncommon condition in which the perception of sensory stimuli is presumably normal but activity is suspended and motor activity is profoundly diminished (catatonia, or catatonic stupor). However, these states, including coma, exist in a continuum, and an alternative practical method of mak ing distinctions between them was given by Fisher, who suggested that a verbal command is required to over come drowsiness whereas a noxious stimulus is required to overcome stupor. This allows for further gradations in the level of consciousness based on the intensity of stimulation that is necessary to produce arousal. Also encompassed in this continuum is the observation that stuporous and drowsy patients may not always be aroused to a fully awake state. There are vari ations in the degree of coma, and the findings and signs depend on the underlying cause of the disorder. In its deepest stages, no meaningful or purposeful reaction of any kind is obtainable and corneal, pupillary, pharyngeal responses are diminished. In lighter stages, sometimes referred to by the ambiguous terms semicoma or obtunda 20). As commented earlier in the discussion of the term "confusion," a relationship between the level of con sciousness and disordered thinking or, content of con sciousness, is evident as patients pass through states of inattention, drowsiness, confusion, stupor, and coma. As mentioned, the depth of coma and stupor may be gauged by the response to externally applied stimuli and is most useful in assessing the direction in which the disease is evolving, particularly when compared in serial examinations. Drowsiness denotes an inability to sustain a wakeful state without the application of external stimuli. Furthermore, in distinction to stupor discussed later, alertness is sustained spontaneously for at least some brief period, without the further neccessity of stimuli. As a rule, some degree of inattentiveness and mild con fusion are coupled with drowsiness, both improving with arousal. The lids droop; there may be snoring, the jaw and limb muscles are slack, and the limbs are relaxed. This state is indistinguishable from light sleep, sometimes with, slow arousal elicited by speaking to the patient or applying a tactile stimulus. Sleep shares a number of other features with the pathologic states of drowsiness, stupor, and coma. These include yawning, closure of the eyelids, ces sation of blinking and reduction in swallowing, upward deviation or divergence or roving movements of the eyes, loss of muscular tone, decrease or loss of tendon reflexes, and even the presence of Babinski signs and irregular respirations, sometimes Cheyne-Stokes in type. Nevertheless, sleeping persons may still respond to unaccustomed stimuli and are capable of some mental activity in the form of dreams that leave traces of memory, thus differing from stupor or coma. The most important difference, of course, is that persons in sleep, when stimulated, can be roused to normal and persistent consciousness.
Mushroom of Spiritual Potency (Reishi Mushroom). Lumigan.
- Dosing considerations for Reishi Mushroom.
- What is Reishi Mushroom?
- Are there any interactions with medications?
- Are there safety concerns?
- How does Reishi Mushroom work?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96871
Related Products
Usage: q.2h.
Additional information:
Tags: lumigan 3 ml order, buy 3 ml lumigan mastercard, buy lumigan 3 ml without prescription, cheap 3 ml lumigan visa
9 of 10
Votes: 57 votes
Total customer reviews: 57
Customer Reviews
Zuben, 49 years: In animals, however, experimental lesions confined to the substantia nigra do not result in tremor; neither do lesions in the striatopal lidum.
Runak, 65 years: In the former, there was a delay of several years between the injury and the start of the movements; these authors also commented on the resistance of this syndrome to drug treatment.
Kurt, 52 years: Affective displays that are excessively labile and poorly controlled or uninhibited are a common manifestation of many cerebral diseases, particularly those involving the corticopontine and corticobulbar pathways.
Kamak, 32 years: The potential for long-term tolerance and brain changes resulting from stimulant use requires further investigation.