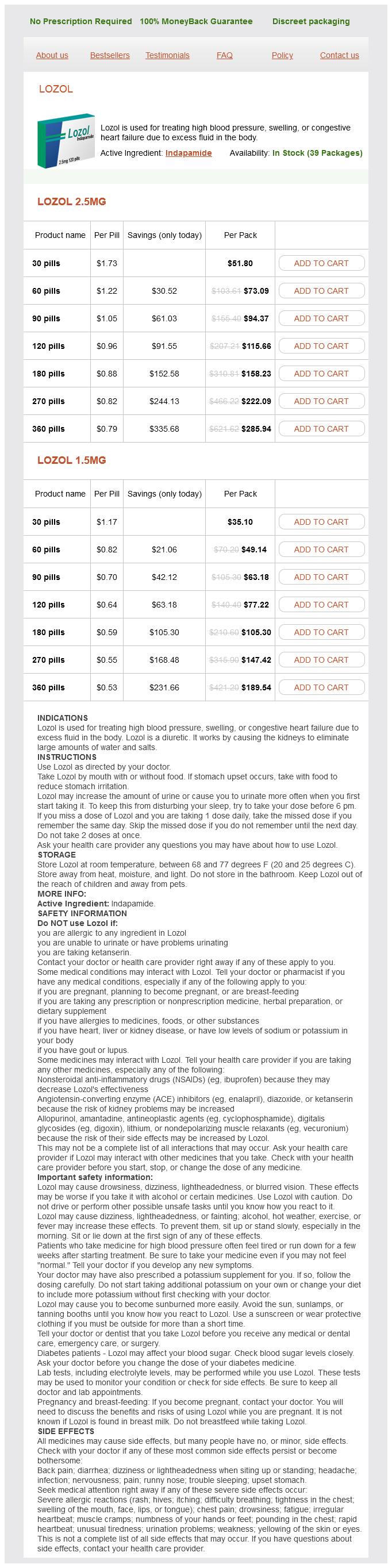
Lozol 2.5mg
- 30 pills - $51.80
- 60 pills - $73.09
- 90 pills - $94.37
- 120 pills - $115.66
- 180 pills - $158.23
- 270 pills - $222.09
- 360 pills - $285.94
Lozol 1.5mg
- 30 pills - $35.10
- 60 pills - $49.14
- 90 pills - $63.18
- 120 pills - $77.22
- 180 pills - $105.30
- 270 pills - $147.42
- 360 pills - $189.54
Lozol dosages: 2.5 mg, 1.5 mg
Lozol packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
Only $0.56 per item
In stock: 681
Description
Potency of Nondepolarizing Neuromuscular Blockers Drug potency is commonly expressed in terms of the dose-response relationship blood pressure levels women order lozol 2.5 mg with visa. This potentiation results mainly in a decrease in the required dosage of neuromuscular blocker and prolongation of both the duration of action of the relaxant and recovery from neuromuscular block. The aminoglycoside antibiotics, the polymyxins, and lincomycin and clindamycin primarily inhibit the prejunctional release of acetylcholine and also depress postjunctional nicotinic acetylcholine receptor sensitivity to acetylcholine. Th s resistance has been attributed to increased clearance,153 increased binding of the neuromuscular blockers to a1-acid glycoproteins, and/or upregulation of neuromuscular acetylcholine receptors. Buffered diffusion causes repetitive binding to and unbinding from receptors, keeping potent drugs such as tubocurarine in the neighborhood of effector sites and potentially lengthening the duration of effect. The fast onset of succinylcholine is related to its rapid metabolism and plasma clearance. Adverse Effects of Neuromuscular Blockers Neuromuscular blocking agents seem to play a prominent role in adverse reactions that occur during anesthesia. The concept of "buffered diffusion" must be invoked to explain the slow recovery of long-acting neuromuscular blockers and to understand biophase kinetics. Administration of tubocurarine is associated with marked ganglion blockade resulting in hypotension; in susceptible patients, manifestations of histamine release such as flushing, hypotension, refle tachycardia, and bronchospasm can be seen. The effect is usually of short duration (1 t o 5 m inutes), is dose related, and is clinically insignificant in healthy patients. Another strategy for maintaining cardiovascular stability involves slow administration of benzylisoquinolinium neuromuscular blocking drugs (over 60 seconds), or the prophylactic use of the combined histamine H1- and H2-receptor antagonists. Drugs for Reversal of Neuromuscular Blockade Acetylcholinesterase at the Neuromuscular Junction At the neuromuscular junction, acetylcholinesterase is the enzyme responsible for rapid hydrolysis of released acetylcholine. It can catalyze acetylcholine hydrolysis at a rate of 4,000 molecules of acetylcholine hydrolyzed per active site per second, which is nearly the rate of diffusion. The acetylcholine that accumulates at the neuromuscular junction after administration of neostigmine competes with the residual molecules of the neuromuscular blocking drug for the available unoccupied nicotinic acetylcholine receptors at the neuromuscular junction. The clinical implication is that neostigmine has a ceiling effect on acetylcholinesterase. Once the inhibition of acetylcholinesterase is complete, administering additional doses of neostigmine will serve no useful purpose because the concentration of acetylcholine that can be produced at the neuromuscular junction is finite. Allergic Reactions Life-threatening anaphylactic (immune-mediated) or anaphylactoid reactions during anesthesia have been estimated to occur in 1 in 1,000 to 1 in 25,000 administrations and are associated with a mortality rate of about 5%. Anaphylactoid reactions are not immune mediated, and represent exaggerated pharmacologic responses in very sensitive individuals, who represent a very small proportion of the population. Cross-reactivity has been reported between neuromuscular blocking drugs and food, cosmetics, disinfectants, and industrial materials. Indeed, administering more neostigmine at this point may in fact worsen neuromuscular recovery.
Syndromes
- Loss of vision
- Doors without cylinder locks should have a heavy bolt or some similar secure device that can be operated only from the inside.
- Abdominal ultrasound
- Throat swelling (may also cause breathing difficulty)
- Urinary tract infections, chronic or recurrent
- Sweating with weight loss
- Avoid shaving the area if possible (if shaving is necessary, use a clean, new razor blade or an electric razor each time)
- Blood calcium
- Symptoms of a heart attack
Predictors of survival after in vivo split liver transplantation: analysis of 110 consecutive patients arrhythmia signs and symptoms buy 1.5 mg lozol free shipping. Living-related liver transplantation in children-a single center evaluation of the outcome of donor candidates and recipients. Techniques for and outcome of liver transplantation in neonates and infants weighing up to 5 kilograms. Liver transplantation in newborn liver failure: treatment for neonatal hemochromatosis. Living donor liver transplantation with reduced monosegments for neonates and small infants. Neonatal liver cirrhosis without iron overload caused by gestational alloimmune liver disease. Neonatal iron overload and tissue siderosis due to gestational alloimmune liver disease. Neonatal hemochromatosis and exchange transfusion: treating the disorder as an alloimmune disease. Cholestasis is a relatively common pediatric disorder, especially in neonates, affecting approximately 1 in every 2,500 live births. Patients with cholestasis frequently progress to end-stage liver disease, often despite initial palliative treatment. The outcome of pediatric patients with cholestasis has improved dramatically with progress in understanding the pathogenesis of cholestasis and the development of therapy targeted to the molecular defect. Biliary atresia is the most common cause of neonatal cholestasis, accounting for up to 25% of the cases; genetic forms of intrahepatic cholestasis account for 25%, 1-antitrypsin deficiency accounts for 10%, other metabolic diseases account for 20%, and viral infections account for 5% of neonatal cholestasis. The goal is prompt identification of treatable disorders such as sepsis, endocrinopathies (including panhypopituitarism and congenital hypothyroidism), and specific metabolic disorders (such as galactosemia, tyrosinemia type I, and inborn errors of bile acid metabolism) to allow initiation of appropriate treatment and to prevent progression of liver damage. Cholestasis associated with severe hepatic synthetic dysfunction points to life-threatening metabolic disorders, such as tyrosinemia type 1 or neonatal iron storage disease. In infants without evidence of infection and with normal synthetic function, early evaluation of the patency of the biliary system is a high priority to recognize biliary atresia. It does not contain discussions of biliary atresia or metabolic and genetic/chromosomal disorders, which are covered elsewhere in this book. These patients may be grouped into "paucity syndromes," which may have different underlying pathological mechanisms, including congenital absence, partial failure to form, atrophy secondary to diminished bile flow, or progressive injury (secondary to immune, viral, or ischemic cause) with secondary disappearance. However, the progressive nature (segmental destructive changes or a progressive decrease in the number of bile ducts per portal tract seen in serial sectioning of biopsy specimens), from the early features of bile duct inflammation to the later observation of paucity, suggests immunological injury to existing ducts (similar to other syndromes of disappearing intrahepatic bile ducts) rather than failure of ducts to develop. Viral hepatitis in the neonate and metabolic liver disease differ from idiopathic neonatal cholestasis by the presence of an identifiable offending agent. Idiopathic neonatal cholestasis implies the existence of an unidentified pathophysiological process associated with inflammatory changes in the liver without evidence of mechanical obstruction. The presence of histological changes of pronounced giant cell transformation of hepatocytes with variable levels of inflammation of unknown etiology in this group of patients resulted in the use of idiopathic neonatal hepatitis to describe this group of patients. Despite the common use, the term implies some type of viral etiology and is best used when a specific agent is identified.
Specifications/Details
If the tumour ruptures arteria century 21 generic lozol 1.5 mg otc, it may lead to formation of pseudomyxoma peritonei and the viscera show extensive adhesions. Appendicectomy at the time of primary surgery prevents pseudomyxoma peritonei, as often mucocele of appendix is known to cause this complication. Tumours of the Surface Epithelium Serous Cystadenoma and Cystadenocarcinoma Serous cystadenoma and cystadenocarcinoma are amongst the most common of cystic ovarian neoplasms, accounting for about 50% of all ovarian tumours; of these, 60Â70% are benign, 15% borderline and 20Â25% are malignant. Serous cystadenomas occur in the third, fourth and fifth decades of life; malignant cystadenocarcinomas tend to occur more frequently with advancing age. Delicate papillary excrescences may be seen on the surface and within the loculi in a benign cyst. In case of serous cystadenocarcinoma, coarse papillary growths spread to the peritoneal surfaces. Histologically, the benign variety shows cystic spaces, and the lining of the tumour consists of tall columnar ciliated epithelium resembling the endosalpinx. The loculi contain a serous straw-coloured fluid, which may be blood stained when malignant transformation occurs. Endometrioid Tumour Endometrioid tumours are mostly malignant and account for about 20% of all ovarian cancers. The tumours are of moderate size, and are essentially solid, with cystic areas in between filled with haemorrhagic fluid. Mesonephroid Tumour Mesonephroid tumour, also called clear cell carcinoma, is an uncommon tumour of the ovary. It is composed of large cuboidal epithelial cells with abundant clear cytoplasm characteristically forming tubules, glands, small cystic spaces lined by clear cells showing large dark nuclei protruding into the lumen (hobnail cells). Brenner Tumour Brenner tumour is an uncommon solid fibro-epithelial tumour accounting for about 1Â2% of all ovarian neoplasms. It is generally unilateral, small to moderate in size, essentially benign and has no endocrine function. The tumour is generally seen in women around menopause, and causes post-menopausal bleeding. Occasionally, it may be associated with ascites and hydrothorax (pseudoMeigs syndrome). Histologically, the tumour shows a background of fibrous tissue-interspersed within it are nests of transitional epithelium (Walthard cell rests). As mentioned earlier, this tumour may be combined with a mucinous adenoma of the ovary. The ascitic fluid is often blood-stained and shows presence of clusters of tumour cells. The tumour cells may spread to the paraaortic lymph nodes, and metastasize to the liver, lungs, gastrointestinal tract and other areas. D Germ Cell Tumours Incidence Germ cell tumours account for 15Â20% of all ovarian tumours.
Feuilles la Fievre (Chanca Piedra). Lozol.
- Are there safety concerns?
- How does Chanca Piedra work?
- Dosing considerations for Chanca Piedra.
- Are there any interactions with medications?
- Urinary tract infections and inflammation, kidney stones, increasing urine, intestinal gas, stimulating the appetite, use as a liver tonic and blood purifier, diabetes, gallstones, colic, stomachache, indigestion, intestinal infections, constipation, dysentery, flu, jaundice, abdominal tumors, fever, pain, syphilis, gonorrhea, malaria, tumors, caterpillar stings, cough, swelling, itching, miscarriage, rectal inflammation, tremors, typhoid, infections of the vagina, anemia, asthma, bronchitis, thirst, tuberculosis, or dizziness.
- Hepatitis B infection.
- What is Chanca Piedra?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96450
Related Products
Usage: q.d.
Additional information:
Tags: lozol 1.5 mg without a prescription, discount 1.5 mg lozol, order lozol 1.5 mg online, purchase lozol 1.5 mg overnight delivery
8 of 10
Votes: 149 votes
Total customer reviews: 149
Customer Reviews
Malir, 56 years: Anagrelide was substituted subsequently because of the development of anemia on hydroxyurea. Intravascular and disseminated peripheral fibroids rarely exist, but are often diagnosed only at laparotomy.
Josh, 50 years: As much as 50% of benign serous epithelial tumours undergo secondary malignant change, but only 5% mucinous cysts undergo malignant transformation. When administered parenterally, heroin acts in a markedly different way than morphine.