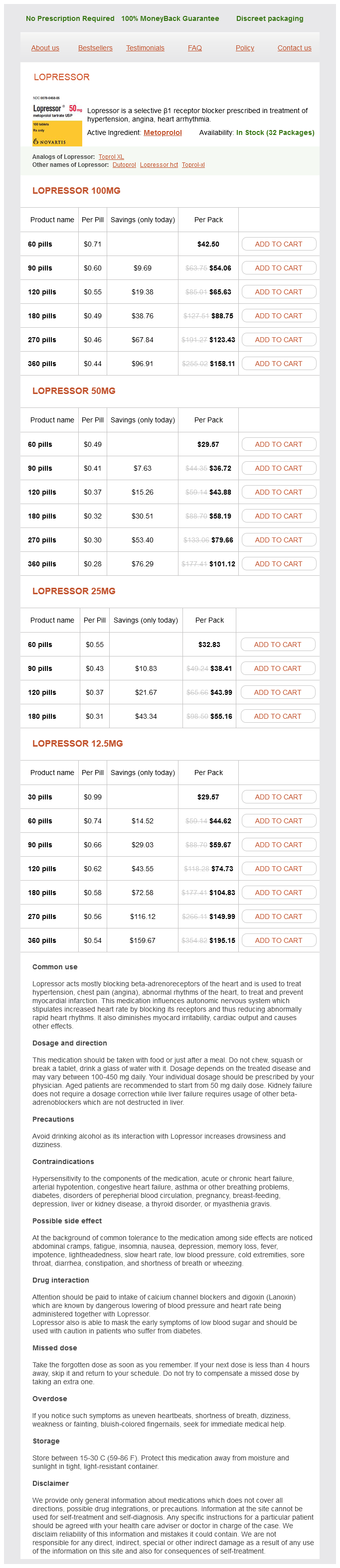
Lopressor 100mg
- 60 pills - $42.50
- 90 pills - $54.06
- 120 pills - $65.63
- 180 pills - $88.75
- 270 pills - $123.43
- 360 pills - $158.11
Lopressor 50mg
- 60 pills - $29.57
- 90 pills - $36.72
- 120 pills - $43.88
- 180 pills - $58.19
- 270 pills - $79.66
- 360 pills - $101.12
Lopressor 25mg
- 60 pills - $32.83
- 90 pills - $38.41
- 120 pills - $43.99
- 180 pills - $55.16
Lopressor 12.5mg
- 30 pills - $29.57
- 60 pills - $44.62
- 90 pills - $59.67
- 120 pills - $74.73
- 180 pills - $104.83
- 270 pills - $149.99
- 360 pills - $195.15
Lopressor dosages: 100 mg, 50 mg, 25 mg, 12.5 mg
Lopressor packs: 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills, 30 pills
Only $0.58 per item
In stock: 699
Description
Conduct and Monitoring of Epidural Analgesia: the Importance of a Dedicated Acute Pain Team the need for safe and effective practice of epidural analgesia on surgical wards was one of the main reasons that acute pain services were established in many hospitals some 20 years ago (Breivik 1993) heart attack lyrics sum 41 lopressor 25 mg buy cheap. Extensive clinical experience has confirmed that these services are essential and that they have made prolonged epidural analgesia more readily available to patients who really need this effective way of controlling the most severe dynamic pain after major surgery. Intravenous opioids and other forms of patient-controlled analgesia became available because of the early efforts of acute pain teams. Basic pharmacological treatment of acute postoperative pain has been upgraded and optimized thanks to the ongoing educational programs, quality assurance, and research activities of acute pain teams in university hospitals (Breivik et al 2007, Counsell et al 2008). Long-Term Epidural Infusions for Chronic Pain the use of external or internal (implanted) pumps may be indicated for cancer-related pain. Experience shows that it is technically difficult to maintain an epidural infusion for prolonged periods because of epidural fibrosis and adhesions. However, the often prolonged epidural infusion is maintained as long as it functions well. In patients with advanced cancer and severe pain and nausea, an epidural infusion using the standard triple epidural infusion (described above) is performed. Intrathecal Infusion Indications for continuous intrathecal administration of an opioid and a local anesthetic (with or without clonidine or adrenaline) are severe cancer pain resistant to traditional treatment, including high doses of oral or parenteral opioids, or when intolerable side effects prevent dose escalation (Raphael and Grady 2008) (Box 37-10). Refractory non-malignant pain may also be an indication for intrathecal treatment in pain management centers where this technique is well established and only when more traditional treatments have not achieved sufficient pain relief or have resulted in intolerable side effects. Ziconotide, an antagonist at N-type voltage-sensitive calcium channels of presynaptic terminals in the dorsal horn of the spinal cord, appears to have a specific effect in chronic pain conditions. It is difficult to titrate but, in selected cases, clearly produces good analgesia without respiratory depression (Raphael and Grady 2008). Alternatives for Epidural Analgesia When the patient has congenital or drug-induced hemostatic disturbances and high risk for intraspinal bleeding provoked by the epidural needle or catheter analgesia, alternative techniques for pain relief must be found (Breivik et al 2010). When there is an evidence base for reduced morbidity and even more so when an epidural may reduce postoperative mortality, it is possible to accept some increased risk for bleeding. However, when such is not the case, even a moderately increased risk for bleeding is a relatively strong contraindication to epidural (and subarachnoid spinal) analgesia. Alternatives for Thoracic Epidural Anesthesia in a Patient with Increased Risk for Bleeding There is no safe alternative nerve block technique: · Intrathecal catheter techniques carry a similar risk for intraspinal bleeding. Therefore, a similar risk for catastrophic bleeding can be expected (Norum and Breivik 2010). This was attempted because the spinal nerve roots appeared inflamed and swollen during operations for prolapsed intervertebral discs. Beneficial effects on pain and function were documented in two-thirds of the patients who had bupivacaine and steroid injections as opposed to one-third of those receiving bupivacaine and saline injections.
Syndromes
- Fatty or oily stools
- Tuberculosis (in the lungs or spread throughout the body)
- Are persistent
- Protect your skin from the sun when you can -- wear protective clothing such as hats, long-sleeved shirts, long skirts, or pants.
- Weight loss or gain
- Mental status changes
- MRI of the brain including special images of the optic nerve
- Trauma
- Your elbow is locked.
- Sore throat
At the trigeminal (brain stem) level, the general response properties of nociceptive neurons in the spinal trigeminal nucleus are similar to those in the spinal dorsal horn (Sessle 2000) hypertension home remedies 12.5 mg lopressor purchase with visa. The trigeminal nerve supplies the masticatory muscles, and activation of trigeminal nociceptors in these muscles leads to motor reflexes and pain sensations (Sessle 2006). Sensitized spinal neurons with input from deep somatic tissue exhibit (1) higher resting activity and responsiveness to muscle stimulation, (2) increased input convergence, and (3) expansion of the spinal target area of the muscle nerve, which is the basis of pain referral. Central sensitization is associated with one or several of the following characteristics. The neuron had low-threshold mechanosensitive input from receptors in the skin of the upper part of the thigh and nociceptive input from both the thoracolumbar fascia and the multifidus muscle. The neuron could also be excited by injecting hypertonic saline into the muscle (B). D, Shift between the recording level (in segment L2) and the location of the receptive fields (close to spinous processes L4 and L5, open circles). Chronic sensitization is independent of further input from the damaged muscle (Sluka et al 2001). Central sensitization can also be induced by repeated intramuscular injection of acidic solutions. Recent findings have demonstrated that even subthreshold synaptic potentials in dorsal horn neurons are sufficient to sensitize the cells. The ischemic contraction is painful and activates muscle nociceptors (Travell et al 1942). In clinical and experimental low back muscle pain, the low back muscle activity was increased in phases in which the electromyogram is normally silent and decreased in phases with normally high electromyographic Central Sensitization by Subthreshold Potentials in Dorsal Horn Neurons Many studies of central sensitization used high-frequency electrical stimulation to elicit long-term potentiation in central neurons. Comparison with results in intact (non-inflamed) rats showed expansion of the target area in animals with myositis. In intact rats, responding neurons were found only in segments L5, L4, and parts of L3 (light blue area with black synapses). In rats with myositis, the target area had expanded and included the entire segments L3 and L6 (orange area). The pressure stimuli were applied with pneumatic forceps that could be closed at a defined force. The pain-related behavior of the animals was determined with a score from no response (0) to strong vocalization (4). In control rats that received an injection of vehicle (phosphate-buffered saline), the pressure pain threshold was 2 bar. The latter finding speaks in favor of inhibition rather than activation of homonymous -motoneurons. In animal experiments using recordings of muscle spindle activity, -motoneurons were not generally facilitated during nociceptive input from muscle (Ro and Capra 2001).
Specifications/Details
Surprisingly, the baseline paw withdrawal threshold to mechanical stimulation does not decrease when only the celiac vagal branches are interrupted (Khasar et al 1998a) blood pressure chart good and bad safe lopressor 12.5 mg. Second, the decrease in the baseline paw withdrawal threshold and bradykinin-induced hyperalgesia following vagotomy takes about 2 weeks to reach a maximum and then remains stable for at least 5 weeks (Khasar et al 1998a, 1998b). Both cannot readily be explained by immediate removal of inhibition from the central nociceptive system. Fourth, bilateral removal or denervation of the adrenal medulla (cutting the sympathetic preganglionic axons that innervate the adrenal medulla) both generates a small increase in the baseline paw withdrawal threshold and attenuates the bradykinin-induced mechanical hyperalgesia when compared with controls. Bradykinin-induced hyperalgesia (decrease in the paw withdrawal threshold) is portrayed in sham-sympathectomized rats (green circles; n = 6 hindpaws), in sympathectomized rats (purple squares; n = 13 hindpaws), and in rats with decentralized lumbar sympathetic chains (preganglionic axons in the lumbar sympathetic chain interrupted 8 days before, blue diamonds; n = 10 hindpaws) (lower inset). Bradykinin was injected intracutaneously at the site of stimulation and at the dose indicated (abscissa scale) in volumes of 2. Both the sham sympathectomy and sympathetic decentralization groups were significantly different from the sympathectomy group. A, Decrease in the paw withdrawal threshold on mechanical stimulation of the dorsum of the rat hindpaw induced by bradykinin (bradykinin-induced behavioral mechanical hyperalgesia) in naïve control (purple circles, n = 26), vagotomized (green triangles, n = 16), and sham-vagotomized (purple squares, n = 18) rats. Post hoc testing shows significant differences in response to bradykinin between vagotomized and normal (P < 0. Cutaneous mechanosensitive nociceptors on the dorsum of the paw are stimulated by a linearly increasing mechanical force. The abscissa scale is the log dose of bradykinin (in nanograms) injected into a volume of 2. The change in the baseline threshold in animals with a denervated adrenal medulla is not significant (Khasar et al 1998b). Slow Time Course of AdrenalineDependent Mechanical Hyperalgesia If the baseline mechanical paw withdrawal threshold and bradykinin hyperalgesia are related to adrenaline released from the adrenal medulla-which is dependent on activity in the sympathetic preganglionic axons innervating the adrenal medulla-one would expect that these changes are reversed when the adrenal medulla is excised or denervated, that adrenaline administered chronically simulates these effects, and that chronic adrenoceptor blockade prevents or attenuates the effect of vagotomy. First, testing of groups of rats over a period of 5 weeks for their mechanical paw withdrawal threshold to 1 ng of bradykinin injected intracutaneously (a dose that does not decrease the threshold to mechanical stimulation in normal rats with intact vagus nerves; see. It reaches its lowest values after 714 days and remains decreased for at least 5 weeks (green triangles in. Reversal of the vagotomy effect after additional denervation of the adrenal medulla (14 days after vagotomy) has a similarly slow time course (blue triangles in. Repeated testing of sham-vagotomized control rats over the same period does not reveal a decrease in the paw withdrawal threshold produced by 1 ng of bradykinin (purple circles in. Second, chronic administration of adrenaline (via a subcutaneously implanted osmotic pump to produce the plasma adrenaline levels seen in adrenal medullaintact rats) generates the same effect as vagotomy: the bradykinin-induced paw withdrawal threshold to mechanical stimulation significantly decreases. This decrease is delayed and reaches its peak effect 14 days after the start of adrenaline infusion. Third, after chronic blockade of 2-adrenoceptors, the decrease in the bradykinin-induced paw withdrawal threshold following vagotomy is significantly attenuated.
French Lavender (Lavender). Lopressor.
- What is Lavender?
- What other names is Lavender known by?
- Are there safety concerns?
- Depression, sleeplessness, agitation, general psychological well-being, loss of appetite, colic, headache, migraine, toothache, acne, nausea, vomiting, cancer, use as a mosquito repellent and insect repellent, and other conditions.
- Hair loss in a condition called alopecia areata when applied to the scalp in combination with other oils.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96813
Related Products
Usage: p.c.
Additional information:
Tags: lopressor 25 mg order fast delivery, generic lopressor 100 mg visa, 100 mg lopressor order with visa, lopressor 25 mg line
10 of 10
Votes: 338 votes
Total customer reviews: 338
Customer Reviews
Wilson, 46 years: Interestingly, in this study psychosocial factors were found to significantly interact with other factors in determining the onset of pain. It is currently available in oral formulation only and is partially absorbed through the small intestine by diffusion and partially facilitated by a saturable carrier-dependent transport mechanism; hence its bioavailability is inversely dependent on dosage. Although studies are limited, existing neurophysiological evidence supports a mirror opponency scheme (Seymour et al 2005). Morning stiffness is a prominent symptom reflecting the profound inflammatory nature of this disease.
Ernesto, 27 years: Detailed knowledge of the features of each route of administration, as well as the suitability of specific compounds via this route, is necessary to treat pain effectively with opioids. Traditionally, these have been divided into diagnostic nerve blocks, prognostic nerve blocks, and therapeutic nerve blocks (Curatolo and Bogduk 2010, Kvarstein 2010); see Box 37-1. It is increasingly becoming apparent that to maximize the yield from trials (which take huge time, effort, and money), a responder analysis should be part of the results. A celiac plexus block relieves the pain as well as the nausea and markedly or completely reduces the amount of opioids needed.
Lukjan, 55 years: Pre-emptive prescription of a stool softener and an artificial saliva mouth spray are useful routine measures. Fischer L, Clemente J, Tambeli C: the protective role of testosterone in the development of temporomandibular joint pain, Journal of Pain 8:437 442, 2007. Cannabinoids Like opioids, cannabinoids have long been used to treat pain (Walker and Huang 2002). Heritability (h2; see later for further discussion) is the proportion of trait variance attributable to genetic inheritance.
Umbrak, 51 years: Further clinical trials have been carried out in patients undergoing total knee and hip arthroplasty, but the entire data have not been published to date. In Krames E, Reig E, editors: Practice of neurology and pain management, Bologna, Italy, 2001, Monduzzi Editore, pp 385389. Astrocytes may respond quickly to stimuli with elevated Ca2+ levels, and they are connected to each other via gap junctions to form extensive networks. A number of alternatives to the conventional readouts described here have been investigated, and there is great interest in developing new approaches.
Ayitos, 35 years: Accounting for individual variations in the neurochemistry of the placebo effect, Brain, Behavior, and Immunity 20:1526, 2006. Results from a large prospective populationbased study, International Journal of Epidemiology 31:12191225, 2002. The use of cryotherapy has controversial data in terms of the efficacy of analgesia. The ascending systems have been reviewed in detail in other portions of this text (see Chapter 12) and several systematic reviews (Willis and Westlund 1997).
Marus, 31 years: Just as conditioning can produce positive expectations and brain changes that reduce pain, it can also produce negative expectations and brain changes that increase pain. The importance of these interrelationships is emphasized by the phenomenon of the central (thalamic) pain syndrome. The cortical synaptic circuitry develops rapidly in the second postnatal week, simultaneous with experience-dependent turnover of dendritic spines. Pain-evoked cerebellar activation is present in anesthetized humans, who are not consciously aware of the pain (Hofbauer et al 2004), thus further suggesting that such activity may be more important in the regulation of afferent nociceptive activity than in the perception of pain.
Peer, 29 years: Since the recruitment of different classes of heat nociceptors and the relative degree of non-nociceptive thermosensor activation depend on the heating profile, minor differences in protocol may be physiologically and pharmacologically relevant. Most interestingly, MrgprA3 has been identified as the receptor mediating chloroquine-induced scratching (Liu et al 2009). Sometimes patients in whom pain is not adequately addressed or treated to their expectations may have features suggestive of addiction, described as pseudo-addiction (Weissman and Haddox 1989). Vanegas H, Schaible H: Effects of antagonists to high-threshold calcium channels upon spinal mechanisms of pain, hyperalgesia and allodynia, Pain 85:918, 2000.
Rune, 41 years: Approximately one-third of individuals with chest pain have normal coronary arteries (Chierchia and Fragasso 1996). In the 1960s, trials of electric stimulation of the sensory thalamus via implanted electrodes for the treatment of chronic neuropathic pain by Mazars and colleagues (1960, 1973) had already commenced at the Hôpital St. One study further specifically examined the cerebral correlates of the altered sense of agency associated with the production of movement in response to hypnotic suggestions (Blakemore et al 2003). Therefore they need not simply analgesia, but suffering, dysfunction, psychosocial factors, and dependence on the health care system need to be addressed as well (Stein 1997).