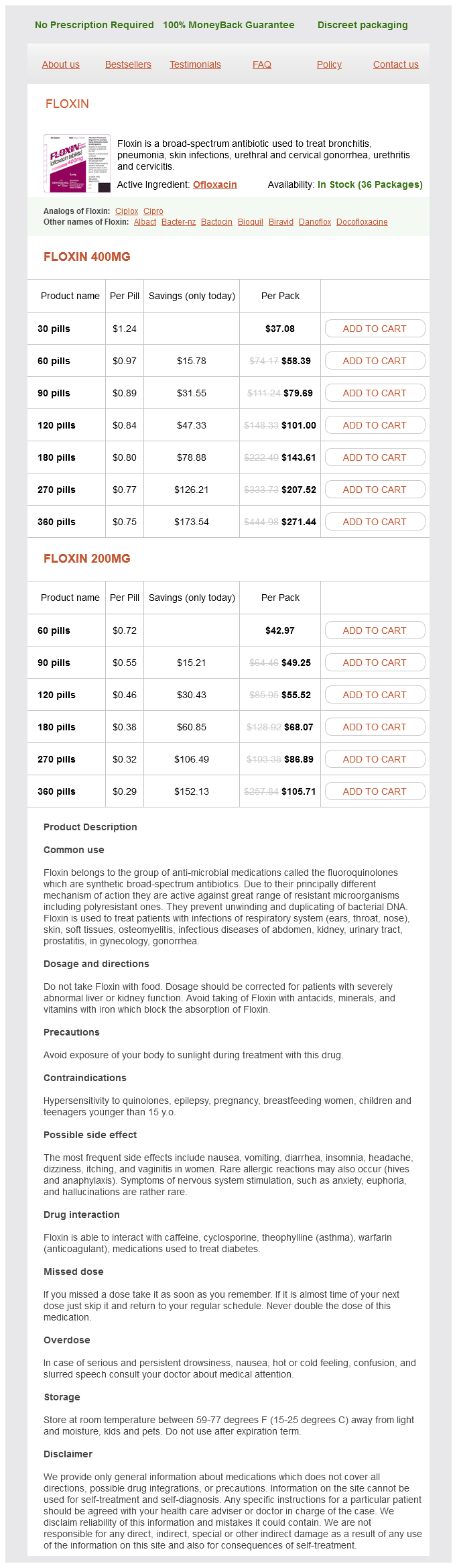
Floxin 400mg
- 30 pills - $37.08
- 60 pills - $58.39
- 90 pills - $79.69
- 120 pills - $101.00
- 180 pills - $143.61
- 270 pills - $207.52
- 360 pills - $271.44
Floxin 200mg
- 60 pills - $42.97
- 90 pills - $49.25
- 120 pills - $55.52
- 180 pills - $68.07
- 270 pills - $86.89
- 360 pills - $105.71
Floxin dosages: 400 mg, 200 mg
Floxin packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
Only $0.31 per item
In stock: 885
Description
For total intravenous anesthesia antibiotic resistance target protein 200 mg floxin amex, the patient is induced with an induction dose of 2 mg/kg of propofol followed by a propofol infusion of 100 to 150 µg/kg/min. Before administering a muscle relaxant, it has traditionally been thought prudent to establish the ability to ventilate the patient by positive pressure through a face mask, although this approach has been questioned. Urgent measures are necessary when the situation deteriorates to acute central airway obstruction. Positive pressure ventilation and suctioning may not be enough in certain situations. Rigid bronchoscopy may be required urgently to force the tube and establish an airway under direct vision. Sedation and Topical Anesthesia thought to be relatively avascular may change to a closed system employing a cuffed laser tube if the lesion is bleeding and there is a risk of soiling the tracheobronchial tree. Conversely, a system employing a cuffed laser tube may have to change during surgery to an open system if the laser tube overlies a lesion, making surgery very difficult or impossible. Topical anesthesia with sedation is suitable for adults who are cooperative and for a short endoscopy period with a flexible bronchoscope. Two distinct mechanisms are accountable for this reduction: decreased respiratory drive and upper airway obstruction. Sedatives alter normal respiratory responses to hypercarbia and hypoxia, thereby decreasing the respiratory drive. Brief hypercarbia and acidosis that may develop under these circumstances are ordinarily inconsequential. However, airway obstruction is a real and more dangerous outcome of sedation because it can quickly lead to oxygen desaturation. A perilous scenario can ensue, with progressively increasing obstruction resulting in total loss of the airway. They include asking the patient to take deep breaths, jaw thrust, chin lift, and insertion of an oral or a nasal airway. However, when these two maneuvers are combined with positive airway pressure, the pharyngeal airway is widened, counteracting airway narrowing. The different types of laser tubes and their relative laser-resistant properties have been discussed. Placement of laser tubes is routine, although care should be taken to prevent traumatizing the laryngeal lesion as the laser tube is passed through the glottis and into the trachea. After the laser tube is in position and the cuff inflated, there is protection of the lower airway from blood and secretions.
Syndromes
- High fasting glucose
- Vaginal ring
- Injury to the small or large intestine
- Weight-bearing exercises -- walking, jogging, playing tennis, dancing
- MRI of the heart can show the connections between the pulmonary vessels
- Checking and rechecking actions (such as turning out the lights and locking the door)
- Stuffing
- Eaten foods such as turkey, turkey dressing, chicken, or eggs that have not been cooked well or stored properly
There is no "ideal anesthetic" for this group of patients antibiotic resistance first discovered order floxin 200 mg on-line, and the perioperative management should be individualized. However, the practitioner should be aware of the effects of anesthetic agents on intracranial dynamics. The preoperative use of midazolam for anxiety in these patients should not cause harm if they are carefully observed. The efficacy of depth of anesthesia was recognized early on as a technique for avoiding intracranial hypertension. Propofol has replaced thiopental (no longer manufactured in the United States) as the induction agent of choice for neuroanesthesia. Ensure adequate depth of anesthesia before intubation attempts or surgical/procedural attempts. If backup position is not possible, use reverse Trendelenburg (avoid hypotension). Avoid rapid infusion of mannitol, which may paradoxically increase intracranial pressure. When vasodilating drugs are used as part of the anesthetic management, the effect of the opioid is consistently that of a vasoconstrictor. The volatile agents, including nitrous oxide, can be considered dose-dependent cerebral vasodilators. The effects on cerebral circulation and metabolism of sevoflurane and desflurane are largely comparable to isoflurane. Sevoflurane is useful in both pediatric and adult patients by allowing inhalation induction without the adverse effects of coughing or breath-holding. The use of topical anesthesia applied to the larynx and trachea can also prevent further response to laryngoscopy and intubation. The obtunded patient with symptoms of intracranial hypertension requires additional attention to detail; avoiding premedication and maneuvers that increase coughing. After loss of consciousness, manual hyperventilation should occur both before and after administration of muscle relaxant. Opioid administration may begin at this time to prevent the sympathetic response to laryngoscopy. Proper airway management is essential to avoid the dual threat of hypoxia and hypercarbia. Early intubation of the head-injured patient is critical and is often established in the field if providers are so trained. It is essential for optimal management of the patient, providing for efficient ventilation and oxygenation, helping to prevent aspiration of gastric contents, and allowing for suction of the lungs and pulmonary toilet. However, patients who are unconscious and breathing adequately may be transported with oxygen by mask throughout their initial assessment.
Specifications/Details
The one-stage prothrombin time described by Quick measures the rate of conversion of prothrombin to thrombin after activation of the extrinsic coagulation pathway in the presence of a tissue extract (thromboplastin) and calcium (Ca++) ions antibiotics for acne when pregnant quality floxin 200 mg. Deficiency of one or more of the liver-produced factors results in a prolonged prothrombin time. Prolongation of the prothrombin time in cholestatic liver disease may result from vitamin K deficiency. Explanations for a prolonged prothrombin time apart from hepatocellular disease or vitamin K deficiency include consumptive coagulopathies, inherited deficiencies of a coagulation factor, or medications that antagonize the prothrombin complex. Assessment of Hepatic Metabolic Capacity Various drugs that undergo purely hepatic metabolism with predictable bioavailability have been used to assess hepatic metabolic capacity. Typically, a metabolite is measured in plasma, urine, or breath following intravenous or oral administration of the parent compound. Antipyrine is metabolized by cytochrome P-450 oxygenase with good absorption after oral 2. In chronic liver disease, good correlation exists between prolongation of the antipyrine half-life 3. Clearance of antipyrine is less impaired in acute liver disease and obstructive jaundice than in 4. Disadvantages of this test include its long half-life in serum, which requires multiple blood administration and elimination entirely by the liver. This test is based on detection of [14C]O2 in breath 2 hours after an oral dose of [14C]dimethyl 2. Excretion is diminished in patients with cirrhosis as well as those with acute liver disease. The test has been used to assess prognosis in patients with alcoholic hepatitis and in cirrhotic 4. A limitation of the aminopyrine breath test is its lack of sensitivity in hepatic dysfunction aminoantipyrine (aminopyrine), which undergoes hepatic metabolism. Caffeine clearance after oral ingestion can be assessed by measuring levels in either saliva or serum; the accuracy appears similar to the [14C]aminopyrine breath test, without the need for a radioisotope. Results are clearly abnormal in clinically severe liver disease, but the test is insensitive in mild 3. Galactose clearance from blood as a result of hepatic phosphorylation can be determined 2. At plasma concentrations >50 mg/dL, removal of galactose reflects hepatic functional mass, whereas at concentrations lower than this plasma level, clearance reflects hepatic blood flow. Galactose clearance is impaired in acute and chronic liver disease as well as in patients with metastatic hepatic neoplasms but is typically unaffected in obstructive jaundice. The oral galactose tolerance test incorporates [14C]galactose with measurement of breath [14C]O2; the results of this breath test correlate with [14C]aminopyrine testing. The test may offer prognostic information about the likelihood of life-threatening complications in cirrhotic patients. The test is easy to perform and has few adverse reactions, although it may be unsuitable for some cardiac patients.
Chromium Polynicotinate (Chromium). Floxin.
- You have a behavioral or psychiatric condition such as depression, anxiety, or schizophrenia.
- You have liver disease.
- Chromium Safety and Side Effects »
- Athletic conditioning.
- Preventing chromium deficiency.
- You have a chromate allergy.
- What is Chromium?
- Chromium Dosing »
- Dosing considerations for Chromium.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96895
Related Products
Usage: q.h.
Additional information:
Tags: effective floxin 200 mg, 200 mg floxin order, discount floxin 200 mg with mastercard, floxin 400 mg buy low price
9 of 10
Votes: 154 votes
Total customer reviews: 154
Customer Reviews
Hauke, 45 years: Hepatolithiasis (recurrent pyogenic cholangitis) (see also Chapter 35) Cholangiocarcinoma develops in 5% to 10% of patients with hepatolithiasis. Usually <1 cm in size; visualized on gallbladder imaging studies (ultrasonography, oral chol4.
Myxir, 42 years: Standard dose regimen: 4-week induction phase followed by maintenance phase using lower doses of the same medications and continued until end point c. Such behavioral treatments appear to provide benefits similar in magnitude to exercise therapy.
Miguel, 46 years: Auscultation of the abdomen is one of the least revealing aspects of the physical examination of a patient with abdominal pain. Essentially, the test determines the adequacy of airflow around an occluded tracheal tube when the cuff is deflated.
Josh, 29 years: It is frequently associated with ascites and expansion of the extravascular albumin pool at the expense of the intravascular albumin pool. The pain of peritoneal inflammation is invariably accentuated by pressure or changes in tension of the peritoneum, whether produced by palpation Obstruction of Hollow Viscera Intraluminal obstruction classically elicits intermittent or colicky abdominal pain that is not as well localized as the pain of parietal peritoneal irritation.