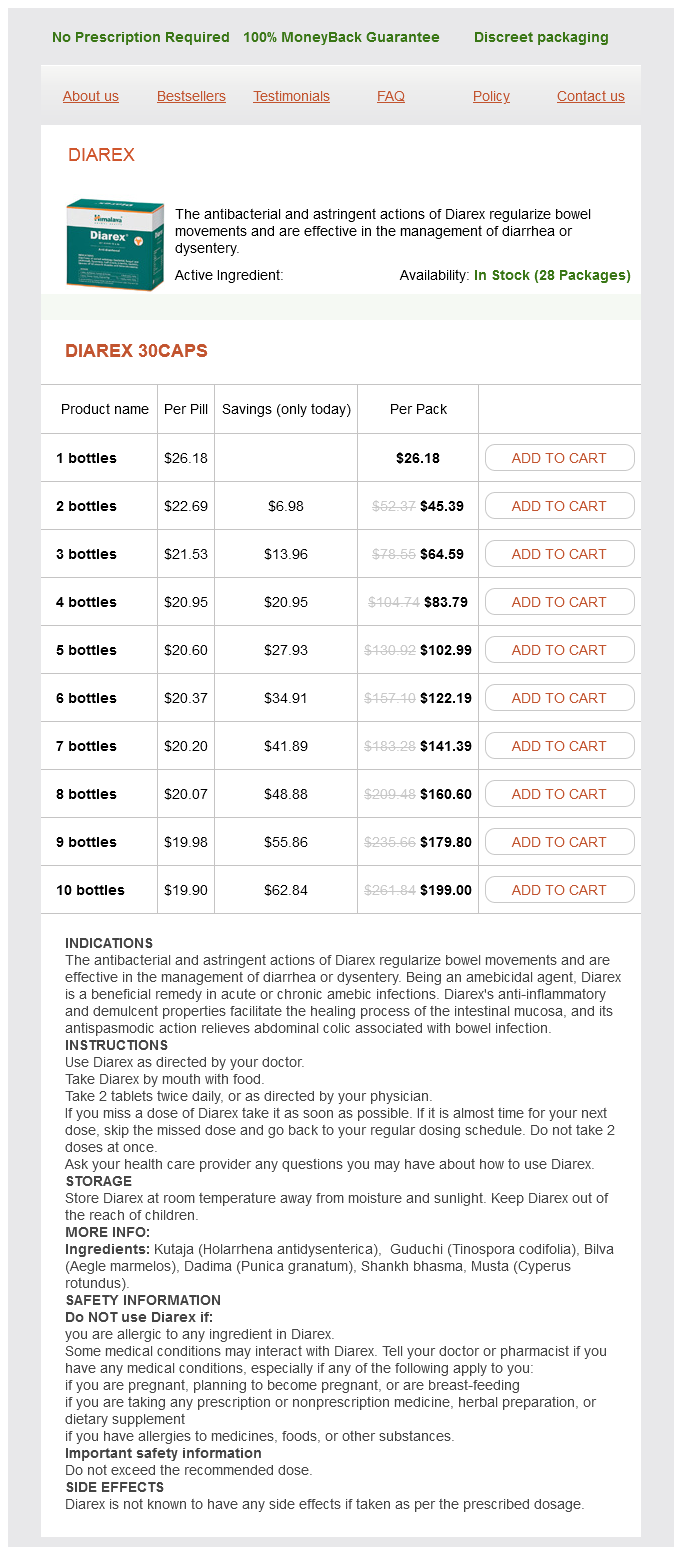
Diarex 30caps
- 1 bottles - $26.18
- 2 bottles - $45.39
- 3 bottles - $64.59
- 4 bottles - $83.79
- 5 bottles - $102.99
- 6 bottles - $122.19
- 7 bottles - $141.39
- 8 bottles - $160.60
- 9 bottles - $179.80
- 10 bottles - $199.00
Diarex dosages: 30 caps
Diarex packs: 1 bottles, 2 bottles, 3 bottles, 4 bottles, 5 bottles, 6 bottles, 7 bottles, 8 bottles, 9 bottles, 10 bottles
Only $21.14 per item
In stock: 537
Description
Prevention of Hypoglycemia Reducing the risk factors for hypoglycemia in diabetes patients involves four basic steps gastritis symptoms fever buy 30 caps diarex with amex. Neonatal Diabetes Neonatal diabetes affects infants and the ability of their bodies to produce or to use insulin. It is monogenic-controlled by a single gene, and develops within the first 6 months of life. This rare disease only occurs in one of every 100,000À500,000 live births, and can be mistaken for type 1 diabetes. The permanent form will never dissipate, while the transient form disappears during infancy, possibly reoccurring later in life. Onset of this condition can be linked to abnormal pancreatic development, and various speeds of beta-cell dysfunction. Pathophysiology of Diabetes Chapter 3 43 the symptoms of neonatal diabetes include the classic symptoms of diabetes mellitus: polydipsia, polyuria, dehydration, dry mouth, dizziness, tiredness, and dark-colored urine. When dehydration is severe, there may be hypotension, a sunken appearance of the eyes, weak pulse, rapid heartbeat, confusion, and fatigue. Also related to neonatal diabetes is intrauterine growth restriction, in which the baby is smaller than normal, and is not growing at a normal weight within the womb. Both permanent and transient neonatal diabetes are genetically inherited from the mother or father of the infant. The causes may be autosomal dominant, autosomal recessive, spontaneous, or X-linked. Transient neonatal diabetes occurs within the first few days to weeks after birth. Insulin dose requirements are usually lower for this form than in permanent neonatal diabetes. Affected infants will relapse in 50% of cases, usually in childhood or young adulthood. Diagnoses of neonatal diabetes are based on intrauterine growth retardation, ketoacidosis, molecular analyses of chromosomes and genes, fasting plasma glucose, oral glucose tolerance, random plasma glucose, and the uniparental disomy test. During the neonatal stage, prognosis is based on severity of the disease and the quickness of its diagnosis and treatment. The first year: type 2 diabetes: an essential guide for the newly diagnosed (the complete first year). Atypical diabetes: pathophysiology, clinical presentations, and treatment options. The type 1 life: a road map for parents of children with newly diagnosed type 1 diabetes. Hyperglycemia: causes, symptoms and treatment options (endocrinology research and clinical developments). Development of the pancreas and neonatal diabetes: 1st Seminar in Developmental Endocrinology, Volume 12.
Syndromes
- Diagnostic staining of the cornea and tear film
- A small amount of prostate enlargement is present in many men over age 40. More than 90% of men over age 80 have the condition.
- Plastics workers
- Need to change any medicine that caused the discharge
- Nervous system
- Fainting or feeling light-headed
- Unexplained fatigue or weight loss
Intraabdominal surgery requires temporary peritoneal rest until the peritoneum has been deemed to have had enough time to recover gastritis diet 91303 30 caps diarex purchase mastercard. Chapter 185 / Treatment of Peritonitis and Other Clinical Complications of Peritoneal Dialysis in the Critically Ill Patient 1125. Staphylococcus aureus prophylaxis and trends in gram-negative infections in peritoneal dialysis patients. Use of aminoglycosides for peritoneal dialysis-associated peritonitis does not affect residual renal function. The association between exit site infection and subsequent peritonitis among peritoneal dialysis patients. Ultrasonography in the management of exit site infections in peritoneal dialysis patients. Examine solute and volume control using peritoneal dialysis in critically ill acute kidney injury patients. Compare peritoneal dialysis with other forms of renal replacement therapy in critically ill acute kidney injury patients in regard to outcomes. Examine the differences in cost for peritoneal dialysis in critically ill acute kidney injury patients. Compare the risks and benefits that peritoneal dialysis may have over other forms of renal replacement therapy in critically ill patients with acute kidney injury. Despite the inherent differences among these modalities, the superiority of one over the other has not been demonstrated clearly. Furthermore, vascular access may be limited, particularly among critically ill infants and small children, or may be difficult to obtain, such as in patients with coagulation disorders or significant vascular disease. The need for anticoagulation, intermittent or continuous, is also a concern because it may raise bleeding risk and is associated with greater utilization of resources for monitoring adequacy of anticoagulation. There was significant heterogeneity between the results of the randomized trials (I2 = 73%, p =. In both studies, rapid correction in metabolic derangement while maintaining an ultrafiltration rate of roughly 2L/day occurred. Obviously, this technique requires either two catheters or a catheter with dual lumens. Urea clearances of 30 to 50 mL/min usually are achieved with this technique, with the potential for even greater clearances. Furthermore, although venous access and peritoneal access can result in infection, central venous access also is associated with the development of venous thrombosis, particularly in the femoral and subclavian veins, putting patients at risk for embolic events.
Specifications/Details
Programmed Cell Death Prevents Oncogenesis the total number of cells in any organ reflects a balance between cell division and cell death gastritis diet 14 buy diarex 30 caps fast delivery. Since many triggers for apoptosis are among the attributes of tumor cells, it is not surprising that those cells often evolve mechanisms to disable it. There are many known pro- and antiapoptotic proteins that interact in a head-spinning number of ways. Thus, promotion of cell proliferation by deregulated production of Myc is usually balanced by increased apoptosis. Induction of apoptosis by Myc acts as a molecular safety valve to block cancer development. This example illustrates the complexity inherent in the control of the on/off switch of apoptosis in cancer development. Wearing several of its many hats, activated p53 upregulates transcription of proapoptotic Bcl-2like proteins and downregulates their prosurvival cousins. It is worth recalling that apoptosis does not elicit florid, cytokine-rich inflammatory responses, but rather that apoptotic cells pass from the world not with a bang but with a whimper-they are quietly removed by macrophages. Their detachment from their extracellular ligands leaves cells excessively susceptible to all manners of proapoptotic stimuli. The prototypical example of the effectiveness of inhibiting apoptosis in human cancer is follicular lymphoma (see Chapter 26). There, the prosurvival protein, Bcl-2, is constitutively activated by a translocation [t(14:8)] that places its expression under the control of the immunoglobulin heavy-chain promoter. As a result, the normal equilibrium between the life and death of B lymphocytes is altered in favor of the former, thus allowing accumulation-or, perhaps, more to the point, insufficient elimination-of excess neoplastic B cells. Some other tumor types, including lung cancer and non-Hodgkin lymphoma, also express excess Bcl-2. Chromosomal translocation is not the only mechanism by which tumor cells increase Bcl-2 expression. Similarly, any impairment of p53 Tumors Stimulate New Blood Vessel Formation (Angiogenesis) Angiogenesis is the formation of new blood vessels from preexisting small blood vessels. In order to grow beyond about 2 mm in diameter, tumors need more nutrient and oxygen supply than preexisting blood vessels can provide. Under homeostatic conditions, there is a fine equilibrium between factors favoring new blood vessel formation and those impeding it. Consequently, endothelial cells turn over slowly, renewing themselves over the course of months or years. Solid tumors often disrupt this equilibrium in favor of new blood vessel formation. Steps in the Formation of New Blood Vessels Tumor angiogenesis begins when existing cells. The process triggered by these chemicals resembles vasculogenesis in embryonic development and follows several steps: 1. Endothelial cells in the area of the interrupted basement membrane proliferate and migrate toward the source of the angiogenic cytokines.
Bergwohlverleih (Arnica). Diarex.
- Dosing considerations for Arnica.
- How does Arnica work?
- Are there safety concerns?
- What is Arnica?
- Reducing pain, swelling, and complications of wisdom tooth removal.
- Are there any interactions with medications?
- Bruises, aches, sprains, insect bites, and sore throats.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96706
Related Products
Usage: q.d.
Additional information:
Tags: 30 caps diarex purchase with mastercard, discount 30 caps diarex free shipping, generic diarex 30 caps visa, diarex 30 caps order fast delivery
9 of 10
Votes: 57 votes
Total customer reviews: 57
Customer Reviews
Spike, 60 years: Very similar drugs in the same class cannot be assumed to share common pharmacokinetics and elimination.
Nafalem, 42 years: In fact, the bypass pump must be primed with solutions to provide an airfree circuit.
Tizgar, 45 years: Thus, equinovarus foot may be caused by uterine wall compression in oligohydramnios or by spinal cord abnormalities that lead to defective innervation and movement of the foot.
Derek, 61 years: Tumor Suppressor Mechanisms Protect from Oncogenesis by Inhibiting Every Tumor Attribute Cells possess complex mechanisms that guard against tumor development.
Aldo, 25 years: Fibrosis itself further alters matrix composition, stiffness and mechanical stress, propagating fibroblast conversion to myofibroblasts and further matrix production.
Irhabar, 33 years: Mechanical circulatory support pathways that maximize post-heart transplant survival.