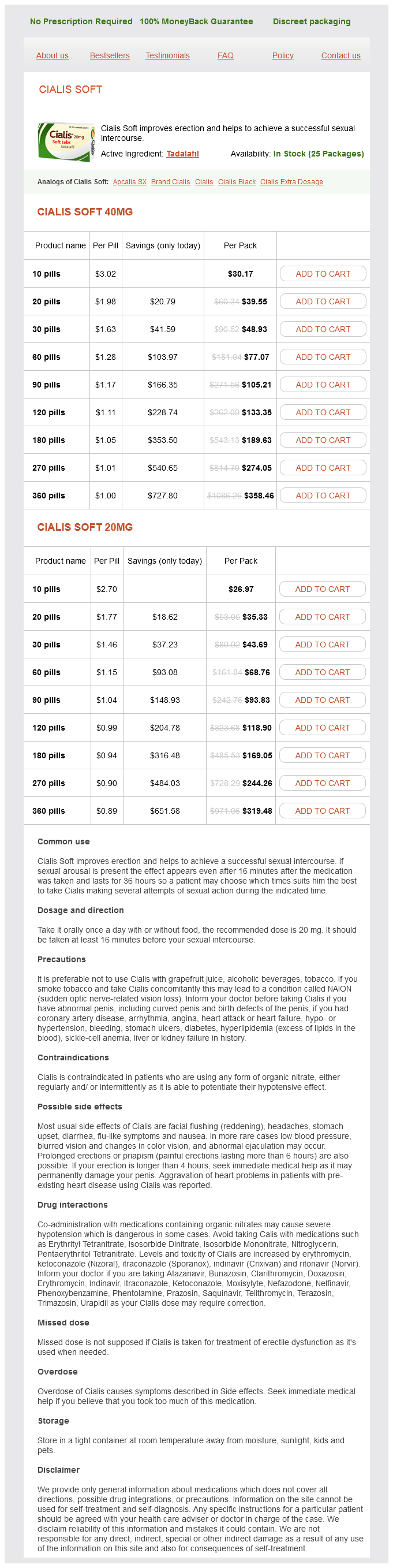
Cialis Soft 40mg
- 10 pills - $30.17
- 20 pills - $39.55
- 30 pills - $48.93
- 60 pills - $77.07
- 90 pills - $105.21
- 120 pills - $133.35
- 180 pills - $189.63
- 270 pills - $274.05
- 360 pills - $358.46
Cialis Soft 20mg
- 10 pills - $26.97
- 20 pills - $35.33
- 30 pills - $43.69
- 60 pills - $68.76
- 90 pills - $93.83
- 120 pills - $118.90
- 180 pills - $169.05
- 270 pills - $244.26
- 360 pills - $319.48
Cialis Soft dosages: 40 mg, 20 mg
Cialis Soft packs: 10 pills, 20 pills, 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
Only $0.94 per item
In stock: 952
Description
Repeated exposure to a mild irritant leads to disruption of the skin barrier and release of proinflammatory mediators by keratinocytes and induction of an eczematous reaction impotence due to diabetes cheap 40 mg cialis soft mastercard. There may be differing effects of skin irritants on different components of the epidermis. The physical nature of the irritant, in particular its pKa, will influence penetration of the epidermis by irritants. Irritants include wet work, where skin is exposed to liquid or occlusive glove use for prolonged periods. According to the German regulation of hazardous substances at the workplace, "wet work" is defined when individuals have their skin exposed to liquids longer than 2 hours per day, or use occlusive gloves longer than 2 hours per day, or clean their hands very often. Other irritants include soaps, detergents, shampoos, solvents, oils, cleaning agents, disinfectants, acids, alkalis, dusts, fiberglass, plants, and a number of miscellaneous chemicals. In addition, the role of physical and environmental irritants has been highlighted, such as heat; sweating under occlusion; friction, such as from handling paper; manual handling; and low humidity. Very often, the semantics are confusing, with the term "eczema" used synonymously with "contact dermatitis. On the other hand, eczema, often but not always associated with atopy, is predominantly of endogenous origin. Of course, environmental factors also may have an important role in atopic dermatitis, which is the subject of Chapter 33. The eczematous lesions generally remain limited to exposure sites, and secondary spread to other areas typically does not occur. The initial development of contact dermatitis often is triggered by a mixture of environmental and occupational exposures, combined with an individual susceptibility to disease, such as the atopic skin diathesis or genetically related skin barrier dysfunction. Skin changes include redness, scaling, blistering, formation of papules or pustules, exudation, and excoriation. In chronic disease, findings may include fissures, lichenification, and hyperkeratosis. This can usually be differentiated on clinical grounds from photoallergy and other photosensitive eruptions: Inspection of the skin will reveal no sparing of shaded areas, such as behind the ears, on the eyelids, and under the chin. Systemic contact dermatitis may occur when sensitized persons are exposed to allergens from routes other than skin exposure, such as orally, intravenously, or by inhalation. Clinical manifestations may include flare-ups of dermatitis in previous sites or of positive patch test site reactions, as well as vesicular hand eczema and "baboon syndrome," which refers to a well-demarcated rash on the buttocks, genital area, and thighs. Causes commonly include metals such as nickel, cobalt, chromate, gold, and mercury. A number of presentations have been described, including erythema multiforme from certain substances such as woods, topical medicaments, and metals; pigmented purpuric eruptions from black rubber, dyes, and medicaments; and lichenoid, bullous, pustular, and other forms of the condition. A thorough history must be ascertained, including the time course of the rash, its relationship to work and hobbies, and the effects of all treatments, which may have complicated the clinical presentation.
Syndromes
- Shortness of breath
- Chills
- Gastroscopy
- Headaches
- Tincture of iodine
- Decreased or no pulse in an arm or leg
- Nonsteroidal anti-inflammatory drugs (NSAIDS) such as ibuprofen to reduce pain and inflammation
- Fluphenazine (Prolixin)
- In the face
- Take the medicines your doctor told you to take with a small sip of water.
Although these compounds are extremely safe erectile dysfunction treatment injection cost generic cialis soft 20 mg line, their use in patients older than 12 years of age is limited. Vilanterol is highly selective for the 2-adrenorecptor and has a 24-hour duration of activity. Sustained-release theophylline has modest bronchodilator activity, and its use in asthma has become limited because of concerns over toxicity and less efficacy than for other long-term controllers (Chapter 94). Toxicity, although rare, can occur, and monitoring of serum theophylline levels is required. In the past decade, there has been tremendous progress with the usage and availability of biologic therapy for asthma. At present, four biologic therapies (omalizumab, mepolizumab, reslizumab, and benralizumab) are approved for use in various phenotypes of asthma (Chapter 91). Omalizumab (anti-IgE) is given as an injectable monoclonal antibody to bind to IgE, thus preventing this antibody from binding to its receptor (Chapter 90). At present, omalizumab is recommended for use in patients (older than 6 years) with severe allergic asthma. All of these biologics have demonstrated benefit in mitigating asthma exacerbations, reducing systemic corticosteroid usage among moderate to severe eosinophilic asthma subjects and with variable improvements in lung function metrics. Other immunomodulators- methotrexate, cyclosporine, and intravenous immunoglobulin-have been evaluated in asthma, with inconsistent effects. Bronchial thermoplasty targets the structural changes, specifically smooth muscle hypertrophy, that occur within the airway smooth muscles of asthmatic patients. At any step level of care, particularly if asthma control is not achieved and maintained, attention should be directed toward patient adherence and techniques in medication use as well as other factors including environmental control. Moreover, alternative diagnoses, such as paradoxical vocal cord motion and eosinophilic granulomatosis with polyangiitis (Churg-Strauss syndrome), should be considered, especially if the patient is not responding to standard therapies. Although current guidelines recommend a stepwise approach to the management of "all" asthma patients, a paradigm shift in asthma management is emerging with a transition toward personalized care such that asthma patients may be broadly phenotyped, and, eventually, endotyped by using clinical and biomarker profiles, which, in turn, would allow selection of targeted therapies to achieve better outcomes, because the chosen intervention is designed to modify patient-specific features or pathways of their disease. Although current information does not provide a full complement of biomarkers to either fully direct or achieve this goal, personalized care for patients can meet the needs of individual variations in asthma and follows the emerging information that multiple asthma phenotypes exist. A brief description of the asthma clinical parameters at each level of step care are discussed in the following sections. This approach may not, however, be effective in all patients, especially those with more severe asthma. The classification of asthma by severity still exists, but step-care Step 1 Care: As-Needed Reliever Inhaler Patients with intermittent asthma have infrequent markers of impairment. In addition, most have few exacerbations, 0 to 1 per year, that require intervention with systemic corticosteroids. Patients with intermittent asthma are still at risk for exacerbations, which, although infrequent, can be severe. In addition, patients beginning step 2 level of treatment usually have a history of 0 to 1 exacerbation in the preceding year. This recommendation has been substantiated by systematic reviews of several well-designed randomized controlled trials.
Specifications/Details
After 2 to 6 weeks of antibiotic treatment impotence means cialis soft 20 mg purchase without prescription, 92% of these children demonstrated a marked improvement of symptoms. Paradoxically, some infectious exposures have also been proposed to prevent the development of asthma. This is suggested by the hygiene hypothesis, which proposed that early life exposures to protective factors. Early exposures to microbial agents such as livestock or probiotics have been studied to assess their ability to influence the development of atopic disease. In addition, the child must meet at least one of the following major conditions or at least 2 of the following minor conditions. Modified Asthma Predictive Index Major Criteria · Parental history of asthma · Physician-diagnosed atopic dermatitis · Allergic sensitization to at least 1 aeroallergen Minor Criteria · Allergic sensitization to milk, egg, or peanuts · Wheezing unrelated to colds · Blood eosinophils 4% Original Asthma Predictive Index Major Criteria · Parental history of asthma · Physician-diagnosed atopic dermatitis Minor Criteria · Physician-diagnosed allergic rhinitis · Wheezing unrelated to colds · Blood eosinophils 4% Asthma Predictive Index Using the risk factors identified from the previously mentioned epidemiologic studies, several predictive scoring approaches have been developed in an effort to identify children at greatest risk for subsequent asthma. Minor criteria were clinician-diagnosed allergic rhinitis, wheezing apart from colds, and eosinophilia in peripheral blood (more than 4% eosinophils). Children with recurrent wheezing and either one major or two minor criteria at 3 years of age were four to seven times more likely to have asthma during later childhood, depending on the frequency of reported wheeze. Genetics Although the molecular basis of several mendelian diseases has been described, genetic studies of common diseases with complex causes have met with less success. In asthma, these evaluations are complicated by multiple childhood asthma phenotypes, inability to replicate significant results, early life exposure assessments, and the complexity of gene-by-environment and gene-by-gene interactions. Because the relationship between genotype and phenotype is more complex than previously thought, accurate study of age-related genetic relationships in asthma requires long-term, longitudinal studies. Several studies have demonstrated an association between genetic variation and the development and severity of asthma. Three longitudinal studies have examined the role of beta-2-adrenoceptor polymorphisms in asthma susceptibility and suggest that the Arg16 allele can be associated with decreased airway function in infancy and the Gly16 allele with asthma symptoms in childhood. Recent evidence suggests that minority residents of inner-city areas are particularly affected by high rates of asthma morbidity and mortality. Racial and ethnic differences for asthma prevalence are well documented (see prevalence, earlier). Among school-aged children, increased asthma prevalence in black children compared with white children remained after adjustment for socioeconomic factors. These racial and ethnic disparities may be related to increased cockroach allergen sensitization in inner city children and ongoing exposure in those sensitized. Depression, stress, and anxiety are well known to be important risk factors for frequent asthma-related emergency room visits and mortality. Severe asthma is also associated with increases in psychological stress and decreases in quality of life creating barriers to adherence to treatment and lifestyle recommendations. Adolescents with severe asthma report missed time with friends, decreased school attendance, teasing from peers regarding their asthma, and reduced involvement in sports, resulting in decreased physical activity related to their illness. However, documenting at least partially reversible airflow obstruction in older children is helpful in establishing a diagnosis of asthma (Table 49.
TC-80 (Ipriflavone). Cialis Soft.
- What is Ipriflavone?
- Treating and preventing osteoporosis (low bone mass) in postmenopausal women.
- Dosing considerations for Ipriflavone.
- How does Ipriflavone work?
- Increasing metabolism in bodybuilders.
- What other names is Ipriflavone known by?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96331
Related Products
Usage: q._h.
Additional information:
Tags: cialis soft 40 mg purchase with mastercard, discount cialis soft 20 mg mastercard, generic cialis soft 20 mg mastercard, purchase 40 mg cialis soft amex
9 of 10
Votes: 59 votes
Total customer reviews: 59
Customer Reviews
Sancho, 44 years: Just as with postsplenectomy sepsis, antibiotics may offer additional protection from serious infection. In the case of differential expression, the expression data for each gene is reduced largely to a mean and variance estimate in each group, ignoring the rich correlation structure among genes.
Rendell, 37 years: Human conjunctival epithelial cells express H1 receptors coupled to phosphatidylinositol turnover and calcium mobilization. Comparison of induced sputum inflammatory profiles between childhood and adult-onset asthma.
Kamak, 53 years: Allergen Immunotherapy Specific allergen immunotherapy is effective in seasonal and perennial allergic rhinitis. The major manifestations are the infection pattern just described and a moderate to severe bleeding tendency secondary to impaired activation of platelet adhesion molecules.
Kippler, 38 years: Neutrophils infiltrate or predominate in the airway in more severe forms of asthma,20 including life-threatening asthma, asthma exacerbations, acute severe asthma, stable persistent asthma, and severe refractory asthma. Third, it is possible to insert chromosomes containing the gene of interest into a foreign cell.