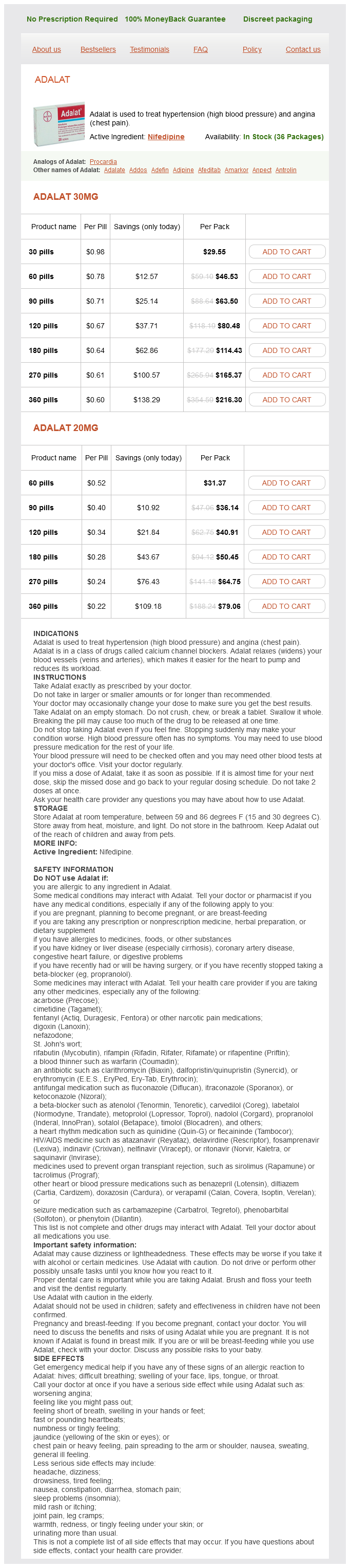
Adalat 30mg
- 30 pills - $29.55
- 60 pills - $46.53
- 90 pills - $63.50
- 120 pills - $80.48
- 180 pills - $114.43
- 270 pills - $165.37
- 360 pills - $216.30
Adalat 20mg
- 60 pills - $31.37
- 90 pills - $36.14
- 120 pills - $40.91
- 180 pills - $50.45
- 270 pills - $64.75
- 360 pills - $79.06
Adalat dosages: 30 mg, 20 mg
Adalat packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
Only $0.23 per item
In stock: 597
Description
Do not treat newborns further without determining what the goals of therapy are 2 arrhythmia nursing care plans discount 20 mg adalat amex. Goal of therapy is not just cessation of seizures but reducing metabolic stress on injured cells 4. Therefore, it is critical to maintain cerebral perfusion, prevent hyperthermia, and deliver energy in parallel with treating seizures 5. Titrate to cessation of seizure activity or burst suppression Seizures continue 1. Anticipate (a) chorea, (b) reduction in need for pressors, (c) spells that mimic seizures, (d) need for repeat monitoring 8. This goal may be achieved by direct and focused attention on variables associated with poor neurological outcome. Neurocritical care in children aims at preventing cerebral hypoxia and ischemia through the avoidance of intracranial hypertension and systemic hypoxia, hypotension, and hypocapnia. Cerebral ischemia may occur as a direct result of inadequate cerebral perfusion, decreased oxygen or glucose supply, increased metabolic demand of the brain, or increased cerebral vascular resistance. For adolescents, the threshold should be 40 to 50 mm Hg, with higher thresholds for older adolescents. The formula 70 mm Hg + (2 × age in years) allows easy calculation of the lower limit (5th percentile) of systolic blood pressure for age. Analysis of the evidence for the lower limit of systolic and mean arterial pressure in children. As new technology becomes available, it may be possible to more effectively determine adequate brain perfusion thresholds in patients with nontraumatic brain injury. Promising new external cooling technology may become available for children in the near future. Propofol in particular has been reported in rare cases to result in refractory shock and metabolic acidosis. In patients recovering from intracranial procedures such as resection of posterior fossa tumors, intermittent careful titration of analgesics is preferred, and nonnarcotic analgesics such as ketorolac can be considered in the absence of obvious contraindications. Finally, although less common, deep venous thrombosis is possible in children with brain disease. Anticoagulation prophylaxis or treatment in children with central venous catheters may be indicated in selected cases, but the risk-benefit ratio in children has not been established. The criteria for establishing brain death in children were published in 1987 in a statement issued by the American Academy of Pediatrics. Examples of such recoverable disorders include drug poisoning, toxicity, metabolic disorder, severe electrolyte disturbances, hypothermia, and shock. The degree of hypothermia that could interfere with a brain death examination is, in general, not well defined. In defining such a threshold at a given institution, consideration should be given to the fact that brainstem reflexes can be lost at a body temperature of 32°C. Because of the difficulty in achieving normothermia in children with loss of brain function, and because of the paucity of data supporting a specific lower limit for temperature, a threshold of 35°C can be considered feasible and appropriate.
Syndromes
- Dizziness
- You have continued symptoms of pain, redness, warmth, or drainage from the area.
- Swollen, tender, or hard lymph nodes
- Unrealistic sexual expectations, which make sex a task instead of a pleasure
- Vascular Birthmarks Foundation -- www.birthmark.org
- You will have blood samples taken in case you need a blood transfusion.
- Blood in the urine
- Lightheadedness
In the original description of this procedure blood pressure during exercise discount adalat 30 mg, the horizontal arm of the craniotomy was placed below the level of the torcula; currently, craniotomies extending above the confluence of the sinuses are carried out in a great percentage of cases to reduce the risk of bleeding from the venous sinuses. Conversely, the craniotomy can be extended to the foramen magnum in the same setting, allowing decompression at the craniovertebral junction. A horizontal tongue-in-groove advancement, including an orbital bar osteotomy and advancement, is usually performed. The upper part of the forehead is remodeled according to each individual case, and two pieces of bone are hinged together to close a widely open fontanelle. In our experience, the frontal advancement in infants should be approximately 2 cm. At first, this needed overcorrection creates an exaggerated frontal bulge, but it is a prerequisite for obtaining a satisfactory long-term result. To attenuate the step-off effect, a small bone graft is placed above the upper part of the nose. B, After early monobloc advancement at 3 years of age, the maxilla is still recessed, but the exophthalmos is corrected. Intraoperative view (A) and three-dimensional reconstruction on computed tomographic scan (B) at the end of the distraction period. Fixation of complex craniofacial reconstructions is now performed primarily with bioabsorbable materials. In infants, titanium miniplates or wire quickly becomes embedded in the growing bone and may migrate intracranially. Therefore, their use in infants is limited or avoided whenever stabilization can be achieved by other means, such as the commonly available bioabsorbable plating systems. The mobilized part includes the lower three fourths of the orbits, the nose, the malar bones, and the upper maxilla. A coronal approach is used to elevate the periosteum around the orbits and at the root of the nose. The osteotomies are made by cutting through the root of the nose and the medial wall, floor, and lateral wall of the orbit with oscillating and reciprocating saws. At the level of the junction of the frontal and malar bones, a section is made on the orbital rim and then downward through the malar bone and the pterygomaxillary space. The maneuver is usually executed from above, especially in children, but it can be performed through an oral approach, especially in adolescents and adults, in whom the bone is thick at this level. Progressive mobilization is achieved, and after the desired position is obtained, fixation is performed by the interposing of bone grafts, wires, and miniplates or absorbable plates between the zygomatic arch and the advanced malar bone. Intramaxillary fixation is used only in older children to ensure proper positioning and is removed after the overall fixation has been performed. This procedure has limited indications in patients with faciocraniosynostosis, for which orbital deepening to correct the exophthalmos is usually necessary.
Specifications/Details
Clinical problems such as slit ventricles pulse pressure 85 adalat 30 mg buy on-line, ventriculomegaly of "low-pressure" hydrocephalus, Chiari malformation and syrinx, and cyst management are examples of these problems. These include adult-onset congenital hydrocephalus or late-onset idiopathic stenosis of the aqueduct, chronic adult hydrocephalus, congenital cysts, and Chiari malformation and syrinx. Although this is a remarkable achievement and one that has contributed countless years of life to those diagnosed, it belies the unfortunate reality that many of these children and their families endure multiple surgeries throughout their early lives. Because the vast majority of these children will survive, only recently has it been recognized that there is an unmet need to provide children with chronic medical conditions, including hydrocephalus, access to physicians and other caregivers capable of providing follow-up care and disease management as they transition from adolescence to adulthood. It is estimated that there are approximately 40,000 individuals between the ages of 18 and 35 with hydrocephalus. Except for a few sites that actively coordinate follow-up care up to and into adulthood, for many of these patients, the care is fragmented. This has predictable consequences in that many of these patients are without a designated provider and then depend on acute care providers for both nonurgent and urgent medical needs, which would be unnecessary with even marginal support. Furthermore, to date there is no formal realization at the national level of the need to identify providers who have the skill set for and interest in seeing these patients, even though the need is immediate. By the time many of these children reach adulthood, they will likely have had numerous surgeries to repair a broken, obstructed, or infected shunt system. Most neurosurgeons will be familiar with the most common issues seen when these young adults present to the emergency department or office with complaints referable to the shunt system. With obstruction, nausea and emesis typically follow, with seizures, lethargy, and eventually coma seen shortly after and sometimes abruptly. Abandoned hardware is not uncommon, and stigmata indicative of multiple cranial surgeries are evident in their scalps, hidden beneath their hair. Some of these patients will have dysmorphically shaped heads and, though less common than in prior eras, cognitive impairment. Many patients with longstanding shunted hydrocephalus will show a collapsed ventricular system despite a blocked catheter, whereas others may have a low-pressure hydrocephalus with ventriculomegaly. It is also important to account for the history of surgical shunting changes and adjustments made in programmable systems. Frequently, the medical records are limited because the original shunt was placed at another institution and the patient may have no recollection of why the shunt was inserted, or why interventions were performed. The nature of the hydrocephalus before treatment was initiated or during times of shunt failure can often be understood by reviewing past imaging. Frequently, transitional patients with a late growth spurt presenting with shunt failure have outgrown their distal catheters.
Ajwan (Celery). Adalat.
- Are there safety concerns?
- Dosing considerations for Celery.
- What is Celery?
- Muscle and joint aches and pains, gout, nervousness, headache, appetite stimulation, exhaustion, fluid retention, regulating bowel movements, use as a sleeping sedative, gas, stimulating menstruation, breast milk reduction, and aiding digestion.
- Are there any interactions with medications?
- How does Celery work?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96850
Related Products
Usage: q.h.
Additional information:
Tags: buy adalat 30 mg fast delivery, purchase adalat 20 mg online, order 30 mg adalat visa, order adalat 20 mg online
9 of 10
Votes: 327 votes
Total customer reviews: 327
Customer Reviews
Gunock, 45 years: It is recommended that myelocystocele repair be carried out within the first 6 months of life in order to minimize neurological losses from spinal cord tethering. Some specific exceptions to this general observation exist; for example, section of the lateral femoral cutaneous nerve might provide long-lasting relief of meralgia paresthetica,83 and section of the ilioinguinal and/or genitofemoral nerves might relieve some inguinal pain syndromes. Digital subtraction cerebral angiogram images demonstrating moyamoya syndrome in a 12-year-old female patient. Regarding angulation in the sagittal plane, studies of the adult subaxial spine by White and Panjabi9,10 demonstrated that the angle between adjacent vertebrae in normal adults is less than 11 degrees and suggested that deformities greater than 11 degrees are considered unstable.
Tarok, 23 years: There is somatotopic organization of axons within the spinothalamic tract; fibers entering from rostral and caudal segments are located in the medial and lateral parts of the tract, respectively. Neuro-endoscopic fenestration of occluded foramen of Monro causing unilateral hydrocephalus. While antibiotic- and antimicrobial-impregnated catheter systems arose from efforts to prevent shunt infection, it should be noted that they do also carry the risk of allowing resistant strains to emerge as the causative microorganisms of shunt infections. For a right-sided approach, the head is first rotated 60 to 75 degrees to the left (more rotation for anteriorly displaced "prefixed" optic chiasm with retrochiasmatic tumors and less rotation for posteriorly displaced "postfixed" optic chiasm as with prechiasmatic tumors), and then the vertex is extended toward the ground with slight forward flexion toward the chin.
Dennis, 56 years: Because their walls are so thin, they are usually identified by the mass effect they exert on surrounding structures. Indeed, many of the rhombomere genes appear to have unique rhombomeric expression profiles. The fourth ventricle is typically small or nonvisualized, flattened and elongated, and extends into the cervical canal. The fascia, subcutaneous tissue, and skin are closed in standard fashion with absorbable sutures.
Javier, 60 years: However, some congenital forms exist in which the maxillary hypoplasia is marked already at birth. Soft tissue closure is done in layers, and although a significant fascial defect may be present, there is sufficient overlying skin to complete a primary closure. In conclusion, clean abdominal surgery should not significantly alter shunt infection rates and thus not necessitate preemptive neurosurgical intervention. Craniovertebral junction abnormalities with hindbrain herniation and syringomyelia: regression of syringomyelia after removal of ventral craniovertebral junction compression.
Varek, 30 years: This vein is the first vein to drain an intracerebral structure and designated the median vein of the prosencephalon. Infection rates following initial cerebrospinal fluid shunt placement across pediatric hospitals in the United States. None of the fractures healed, all four of the patients were left with ossification defects, but none of the patients had progressive neurological problems. In these patients, and in those with multiple abdominal surgeries (shunting and otherwise), collaboration with general surgeons is advantageous.
Spike, 48 years: Successful treatment of an arteriovenous malformation by chemical embolization with estrogen followed by conventional radiotherapy. These entities are seen most commonly in the lumbosacral area and may be apparent only with the aid of magnification. Cutaneous lesions in occult spinal dysraphism: correlation with intraspinal findings. A 15-year-old patient with type 1 mucopolysaccharidosis presented with myelopathic symptoms.